

Axitinib is an active treatment for all histologic subtypes of advanced thyroid cancer: results from a phase II study
- PMID: 18541897
- PMCID: PMC4859206
- DOI: 10.1200/JCO.2007.15.9566
Axitinib is an active treatment for all histologic subtypes of advanced thyroid cancer: results from a phase II study
Abstract
Purpose: Patients with advanced, incurable thyroid cancer not amenable to surgery or radioactive iodine ((131)I) therapy have few satisfactory therapeutic options. This multi-institutional study assessed the activity and safety of axitinib, an oral, potent, and selective inhibitor of vascular endothelial growth factor receptors (VEGFR) 1, 2, and 3 in patients with advanced thyroid cancer.
Patients and methods: Patients with thyroid cancer of any histology that was resistant or not appropriate for (131)I were enrolled onto a single-arm phase II trial to receive axitinib orally (starting dose, 5 mg twice daily). Objective response rate (ORR) by Response Evaluation Criteria in Solid Tumors was the primary end point. Secondary end points included duration of response, progression-free survival (PFS), overall survival, safety, and modulation of soluble (s) VEGFR.
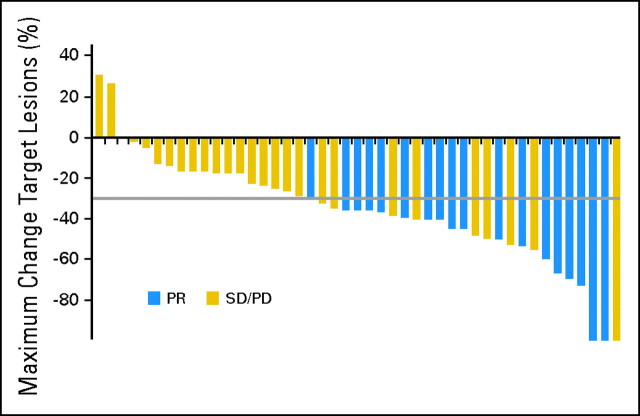
Results: Sixty patients were enrolled. Partial responses were observed in 18 patients, yielding an ORR of 30% (95% CI, 18.9 to 43.2). Stable disease lasting > or = 16 weeks was reported in another 23 patients (38%).
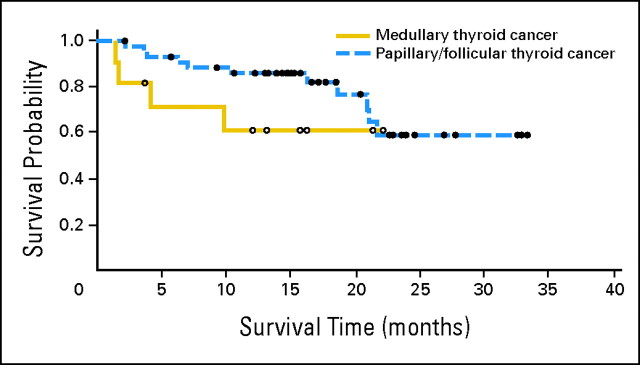
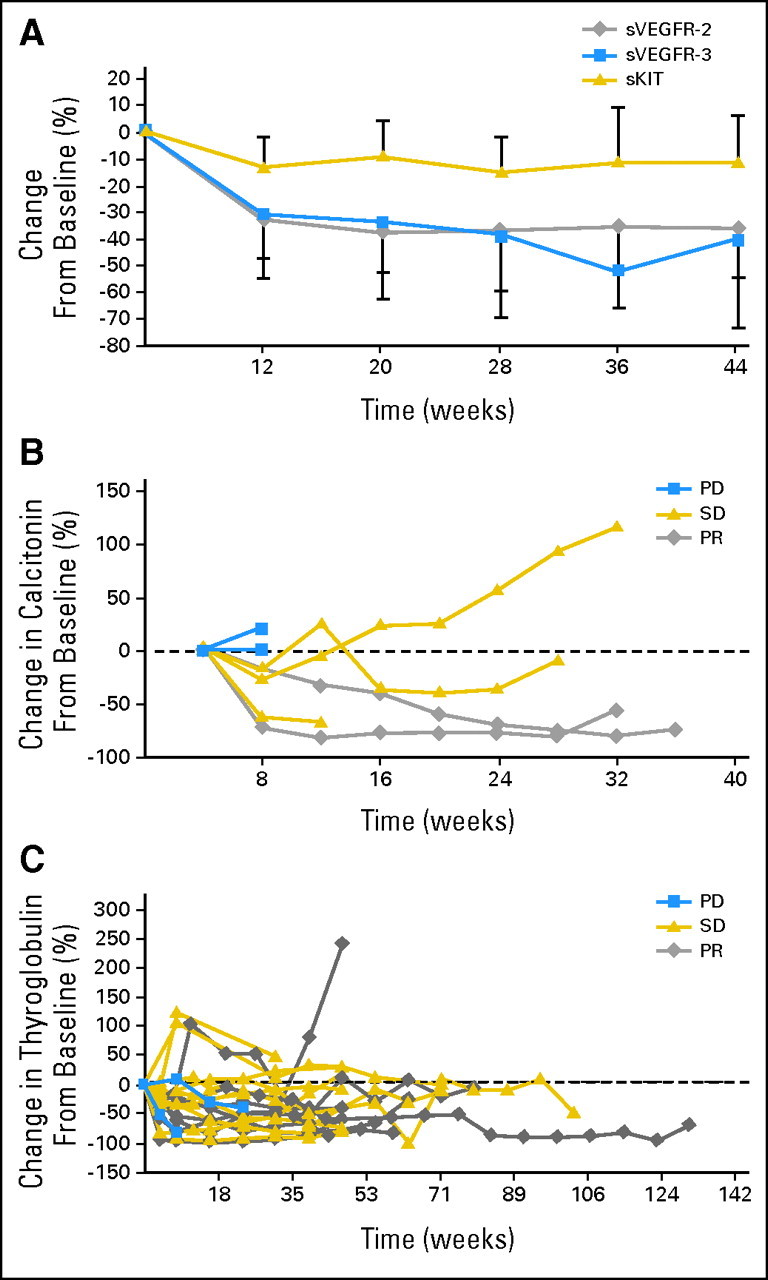
Objective: responses were noted in all histologic subtypes. Median PFS was 18.1 months (95% CI, 12.1 to not estimable). Axitinib was generally well tolerated, with the most common grade > or = 3 treatment-related adverse event being hypertension (n = 7; 12%). Eight patients (13%) discontinued treatment because of adverse events. Axitinib selectively decreased sVEGFR-2 and sVEGFR-3 plasma concentrations versus sKIT, demonstrating its targeting of VEGFR.
Conclusion: Axitinib is a selective inhibitor of VEGFR with compelling antitumor activity in all histologic subtypes of advanced thyroid cancer.
Figures
Comment in
-
Refractory thyroid cancer: a paradigm shift in treatment is not far off.J Clin Oncol. 2008 Oct 10;26(29):4701-4. doi: 10.1200/JCO.2008.17.3682. Epub 2008 Jun 9. J Clin Oncol. 2008. PMID: 18541893 No abstract available.
References
-
- Parkin DM, Bray F, Ferlay J, et al: Global cancer statistics, 2002. CA Cancer J Clin 55::74,2005-108, - PubMed
-
- Davies L, Welch HG: Increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA 295::2164,2006-2167, - PubMed
-
- Gilliland FD, Hunt WC, Morris DM, et al: Prognostic factors for thyroid carcinoma: A population-based study of 15,698 cases from the Surveillance, Epidemiology and End Results (SEER) program 1973-1991. Cancer 79::564,1997-573, - PubMed
-
- Jemal A, Siegel R, Ward E, et al: Cancer statistics, 2008. CA Cancer J Clin 58::71,2008-96, - PubMed
-
- Sherman SI: Thyroid carcinoma. Lancet 361::501,2003-511, - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
