

Value of risk stratification to increase the predictive validity of HbA1c in screening for undiagnosed diabetes in the US population
- PMID: 18543044
- PMCID: PMC2517991
- DOI: 10.1007/s11606-008-0661-6
Value of risk stratification to increase the predictive validity of HbA1c in screening for undiagnosed diabetes in the US population
Abstract
Background: Opportunistic screening using hemoglobin A1c (HbA1c) may improve detection of undiagnosed diabetes but remains controversial.
Objective: To evaluate the predictive validity of HbA1c as a screening test for undiagnosed diabetes in a risk-stratified sample of the US population.
Design: Weighted cross-sectional analysis of diabetes risk factors, HbA1c, and fasting plasma glucose (FPG) in National Health and Nutrition Examination Survey (NHANES), 1999-2004.
Subjects: Six thousand seven hundred and twenty-three NHANES participants from morning examination session, aged > or = 18 years and without prior physician-diagnosed diabetes.
Measurements: HbA1c and undiagnosed diabetes defined by FPG > or = 7.0 mmol/l (126 mg/dl).
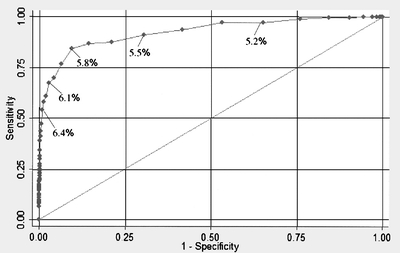
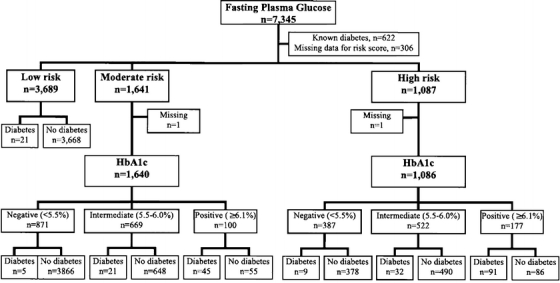
Results: The estimated prevalence of undiagnosed diabetes in the US population was 2.8% (5.5 million people). HbA1c had strong correlation with undiagnosed diabetes, with an area under the receiver-operating characteristic curve of 0.93. Independent predictors of undiagnosed diabetes were older age, male sex, black race, hypertension, elevated waist circumference, elevated triglycerides, and low high-density lipoprotein cholesterol. We derived a risk score for undiagnosed diabetes and stratified participants into low (0.44% prevalence), moderate (4.1% prevalence), and high (11.1% prevalence) risk subgroups. In moderate and high risk groups, a threshold HbA1c value > or = 6.1% identified patients requiring confirmatory FPG; HbA1c < or = 5.4% identified patients for whom diabetes could be reliably excluded. Intermediate HbA1c (5.5-6.0%) may exclude diabetes in moderate, but not high risk groups).
Conclusions: Risk stratification improves the predictive validity of HbA1c in screening for undiagnosed diabetes in the US population. Although opportunistic screening with HbA1c would improve detection of undiagnosed diabetes, cost-effectiveness studies are needed before implementation of specific screening strategies using HbA1c.
Figures
Similar articles
-
Combined use of fasting plasma glucose and glycated hemoglobin A1c in the screening of diabetes and impaired glucose tolerance.Acta Diabetol. 2010 Sep;47(3):231-6. doi: 10.1007/s00592-009-0143-2. Epub 2009 Sep 17. Acta Diabetol. 2010. PMID: 19760291
-
Prevalence of Prediabetes and Undiagnosed Diabetes in Canada (2007-2011) According to Fasting Plasma Glucose and HbA1c Screening Criteria.Diabetes Care. 2015 Jul;38(7):1299-305. doi: 10.2337/dc14-2474. Epub 2015 Apr 7. Diabetes Care. 2015. PMID: 25852207
-
Screening and Diagnosis of Prediabetes and Diabetes in US Children and Adolescents.Pediatrics. 2020 Sep;146(3):e20200265. doi: 10.1542/peds.2020-0265. Epub 2020 Aug 10. Pediatrics. 2020. PMID: 32778539 Free PMC article.
-
Physical and Metabolic Characteristics of Persons With Diabetes and Prediabetes.In: Cowie CC, Casagrande SS, Menke A, Cissell MA, Eberhardt MS, Meigs JB, Gregg EW, Knowler WC, Barrett-Connor E, Becker DJ, Brancati FL, Boyko EJ, Herman WH, Howard BV, Narayan KMV, Rewers M, Fradkin JE, editors. Diabetes in America. 3rd edition. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases (US); 2018 Aug. CHAPTER 9. In: Cowie CC, Casagrande SS, Menke A, Cissell MA, Eberhardt MS, Meigs JB, Gregg EW, Knowler WC, Barrett-Connor E, Becker DJ, Brancati FL, Boyko EJ, Herman WH, Howard BV, Narayan KMV, Rewers M, Fradkin JE, editors. Diabetes in America. 3rd edition. Bethesda (MD): National Institute of Diabetes and Digestive and Kidney Diseases (US); 2018 Aug. CHAPTER 9. PMID: 33651536 Free Books & Documents. Review.
-
Screening for dysglycaemia in dental primary care practice settings: systematic review of the evidence.Int Dent J. 2018 Dec;68(6):369-377. doi: 10.1111/idj.12405. Epub 2018 May 8. Int Dent J. 2018. PMID: 29740815 Free PMC article.
Cited by
-
Diabetes in the Emergency Department and Hospital: Acute Care of Diabetes Patients.Curr Emerg Hosp Med Rep. 2013 Mar 1;1(1):1-9. doi: 10.1007/s40138-012-0007-x. Curr Emerg Hosp Med Rep. 2013. PMID: 23997994 Free PMC article. No abstract available.
-
Management of Hyperglycemia and Diabetes in the Emergency Department.Curr Diab Rep. 2017 Aug;17(8):56. doi: 10.1007/s11892-017-0883-2. Curr Diab Rep. 2017. PMID: 28646357 Review.
-
Predicting risk of type 2 diabetes in England and Wales: prospective derivation and validation of QDScore.BMJ. 2009 Mar 17;338:b880. doi: 10.1136/bmj.b880. BMJ. 2009. PMID: 19297312 Free PMC article.
-
Guidelines for the primary prevention of stroke: a statement for healthcare professionals from the American Heart Association/American Stroke Association.Stroke. 2014 Dec;45(12):3754-832. doi: 10.1161/STR.0000000000000046. Epub 2014 Oct 28. Stroke. 2014. PMID: 25355838 Free PMC article.
-
An investigation into the relationship between plain water intake and glycated Hb (HbA1c): a sex-stratified, cross-sectional analysis of the UK National Diet and Nutrition Survey (2008-2012).Br J Nutr. 2017 Nov 28;116(10):1770-1780. doi: 10.1017/S0007114516003688. Epub 2016 Nov 10. Br J Nutr. 2017. PMID: 27831459 Free PMC article.
References
-
- Centers for Disease Control and Prevention. National diabetes fact sheet: general information and national estimates on diabetes in the United States, 2005. Rev ed. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, 2005.
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.2337/dc06-0062', 'is_inner': False, 'url': 'https://doi.org/10.2337/dc06-0062'}, {'type': 'PubMed', 'value': '16732006', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/16732006/'}]}
- Cowie CC, Rust KF, Byrd-Holt DD, et al. Prevalence of diabetes and impaired fasting glucose in adults in the US population. Diabetes Care. 2006; 29:1263–8. - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.2337/diacare.15.7.815', 'is_inner': False, 'url': 'https://doi.org/10.2337/diacare.15.7.815'}, {'type': 'PubMed', 'value': '1516497', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/1516497/'}]}
- Harris MI, Klein R, Welborn TA, Knullman MW. Onset of NIDDM occurs at least 4–7 years before clinical diagnosis. Diabetes Care. 1992;15:815–9. - PubMed
-
- US Department of Health and Human Services. Healthy people 2010. 2nd ed. With understanding and improving health and objectives for improving health. Section 5: Diabetes. Washington, DC: US Government Printing Office, November 2000.
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '12558361', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/12558361/'}]}
- US Preventive Services Task Force. Screening for type 2 diabetes mellitus in adults: Recommendations and rationale. Ann Intern Med. 2003;1:212–4. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
