

Lower growth hormone and higher cortisol are associated with greater visceral adiposity, intramyocellular lipids, and insulin resistance in overweight girls
- PMID: 18544645
- PMCID: PMC2519763
- DOI: 10.1152/ajpendo.00052.2008
Lower growth hormone and higher cortisol are associated with greater visceral adiposity, intramyocellular lipids, and insulin resistance in overweight girls
Abstract
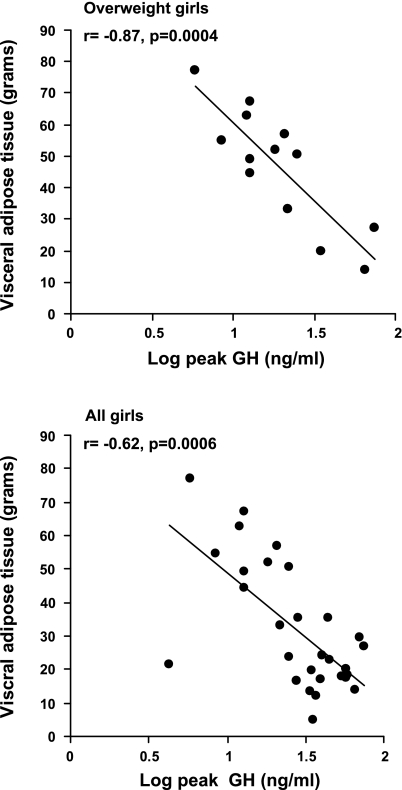
Although body composition, insulin sensitivity, and lipids are markedly altered in overweight adolescents, hormonal associations with these parameters have not been well characterized. Growth hormone (GH) deficiency and hypercortisolemia predispose to abdominal adiposity and insulin resistance, and GH secretion is decreased in obese adults. We hypothesized that low-peak GH on the GH-releasing hormone (GHRH)-arginine stimulation test and high cortisol in overweight adolescents would be associated with higher regional fat, insulin resistance, and lipids. We examined the following parameters in 15 overweight and 15 bone age-matched control 12- to 18-yr-old girls: 1) body composition using dual-energy X-ray absorptiometry and MR [visceral and subcutaneous adipose tissue at L(4)-L(5) and soleus intramyocellular lipid ((1)H-MR spectroscopy)], 2) peak GH on the GHRH-arginine stimulation test, 3) mean overnight GH and cortisol, 4) 24-h urinary free cortisol (UFC), 5) fasting lipids, and 6) an oral glucose tolerance test. Stepwise regression was the major tool employed to determine relationships between measured parameters. Log peak GH on the GHRH-arginine test was lower (P = 0.03) and log UFC was higher (P = 0.02) in overweight girls. Log mean cortisol (overnight sampling) was associated positively with subcutaneous adipose tissue and, with body mass index standard deviation score, accounted for 92% of its variability, whereas log peak GH and body mass index standard deviation score accounted for 88% of visceral adipose tissue variability and log peak GH for 34% of the intramyocellular lipid variability. Log mean cortisol was independently associated with log homeostasis model assessment of insulin resistance, LDL, and HDL and explained 49-59% of the variability. Our data indicate that lower peak GH and higher UFC in overweight girls are associated with visceral adiposity, insulin resistance, and lipids.
Figures


References
-
- Aimaretti G, Baffoni C, Bellone S, Di Vito L, Corneli G, Arvat E, Benso L, Camanni F, Ghigo E. Retesting young adults with childhood-onset growth hormone (GH) deficiency with GH-releasing-hormone-plus-arginine test. J Clin Endocrinol Metab 85: 3693–3699, 2000. - PubMed
-
- Ballerini MG, Ropelato MG, Domene HM, Pennisi P, Heinrich JJ, Jasper HG. Differential impact of simple childhood obesity on the components of the growth hormone-insulin-like growth factor (IGF)-IGF binding proteins axis. J Pediatr Endocrinol Metab 17: 749–757, 2004. - PubMed
-
- Barat P, Gayard-Cros M, Andrew R, Corcuff JB, Jouret B, Barthe N, Perez P, Germain C, Tauber M, Walker BR, Mormede P, Duclos M. Truncal distribution of fat mass, metabolic profile and hypothalamic-pituitary-adrenal axis activity in prepubertal obese children. J Pediatr 150: 535–539, 2007. - PubMed
-
- Baum HB, Biller BM, Finkelstein JS, Cannistraro KB, Oppenhein DS, Schoenfeld DA, Michel TH, Wittink H, Klibanski A. Effects of physiologic growth hormone therapy on bone density and body composition in patients with adult-onset growth hormone deficiency. A randomized, placebo-controlled trial. Ann Intern Med 125: 883–890, 1996. - PubMed
-
- Baumann G Growth hormone and its disorders. In: Principles and Practice of Endocrinology and Metabolism (3rd ed.), edited by Becker KL. Philadelphia, PA: Lippincott Williams & Wilkins, 2001, p. 129–144.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical