

Phosphorylated TDP-43 in frontotemporal lobar degeneration and amyotrophic lateral sclerosis
- PMID: 18546284
- PMCID: PMC2674108
- DOI: 10.1002/ana.21425
Phosphorylated TDP-43 in frontotemporal lobar degeneration and amyotrophic lateral sclerosis
Abstract
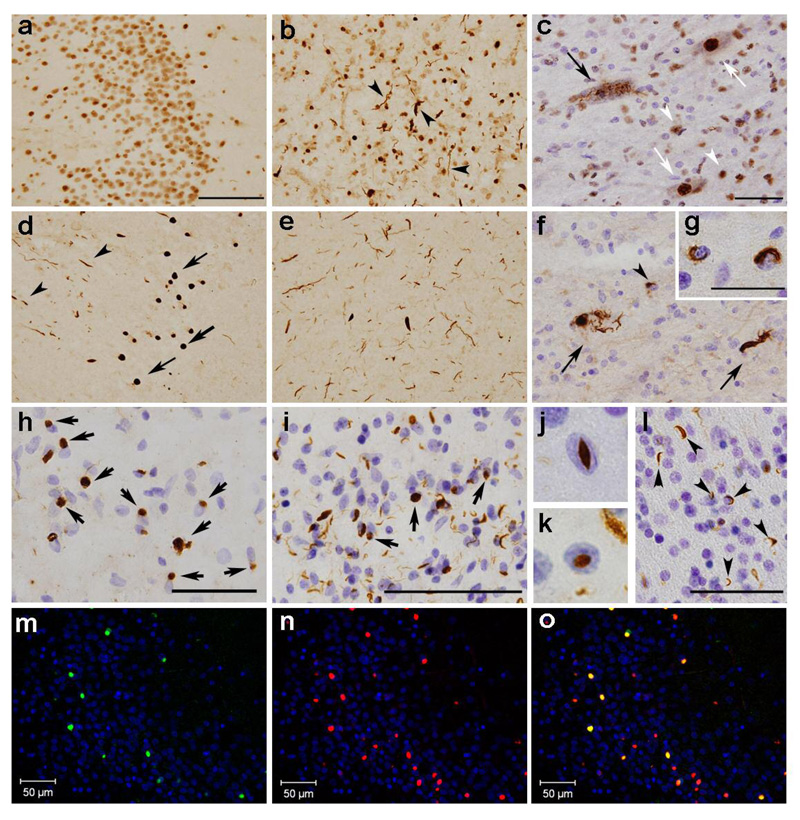
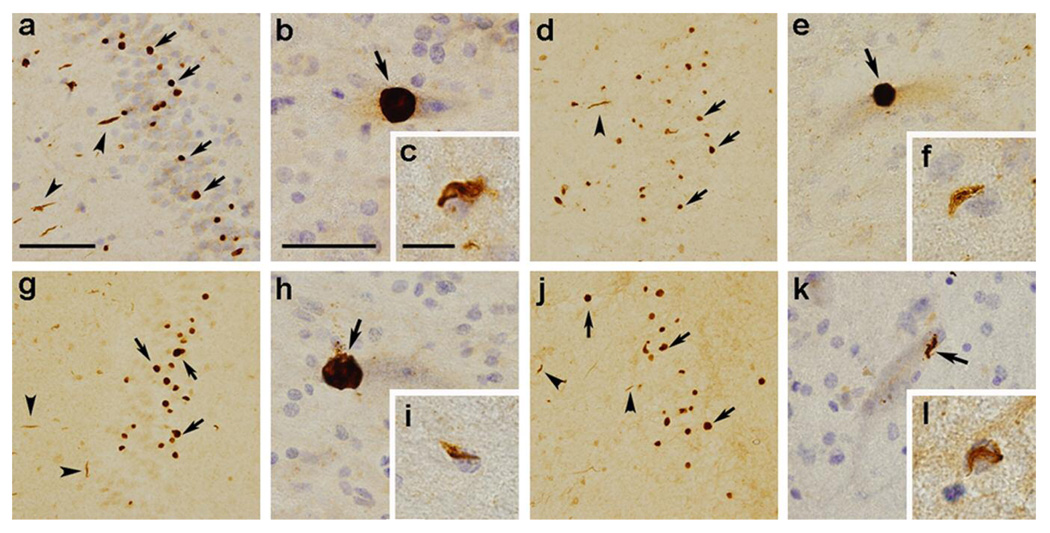
Objective: TAR DNA-binding protein of 43kDa (TDP-43) is deposited as cytoplasmic and intranuclear inclusions in brains of patients with frontotemporal lobar degeneration with ubiquitinated inclusions (FTLD-U) and amyotrophic lateral sclerosis (ALS). Previous studies reported that abnormal phosphorylation takes place in deposited TDP-43. The aim of this study was to identify the phosphorylation sites and responsible kinases, and to clarify the pathological significance of phosphorylation of TDP-43.
Methods: We generated multiple antibodies specific to phosphorylated TDP-43 by immunizing phosphopeptides of TDP-43, and analyzed FTLD-U and ALS brains by immunohistochemistry, immunoelectron microscopy, and immunoblots. In addition, we performed investigations aimed at identifying the responsible kinases, and we assessed the effects of phosphorylation on TDP-43 oligomerization and fibrillization.
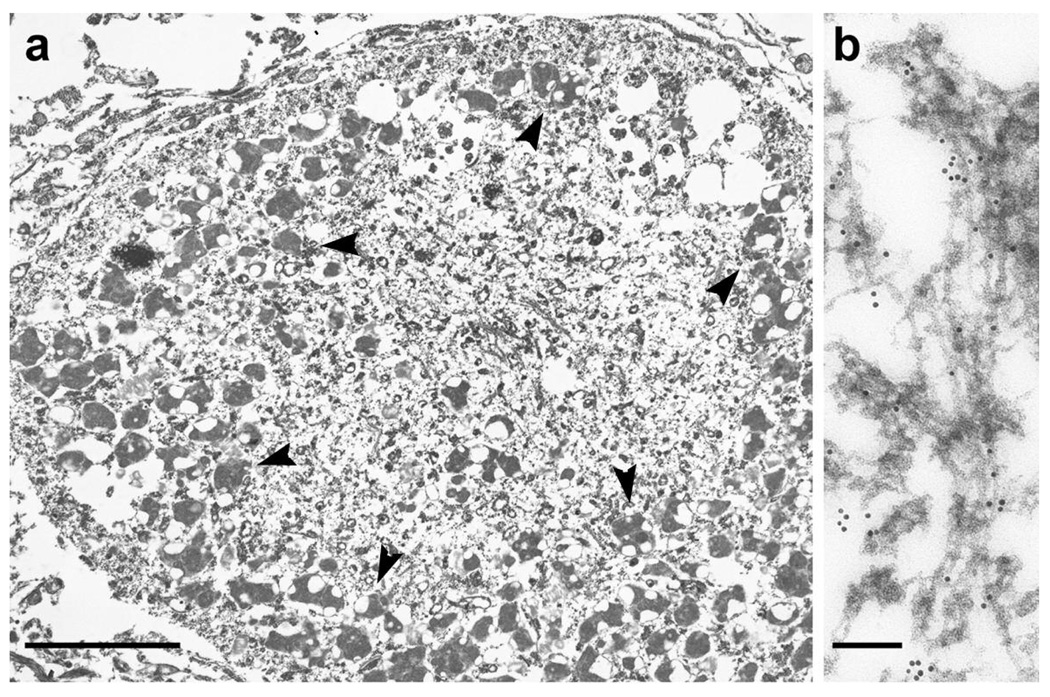
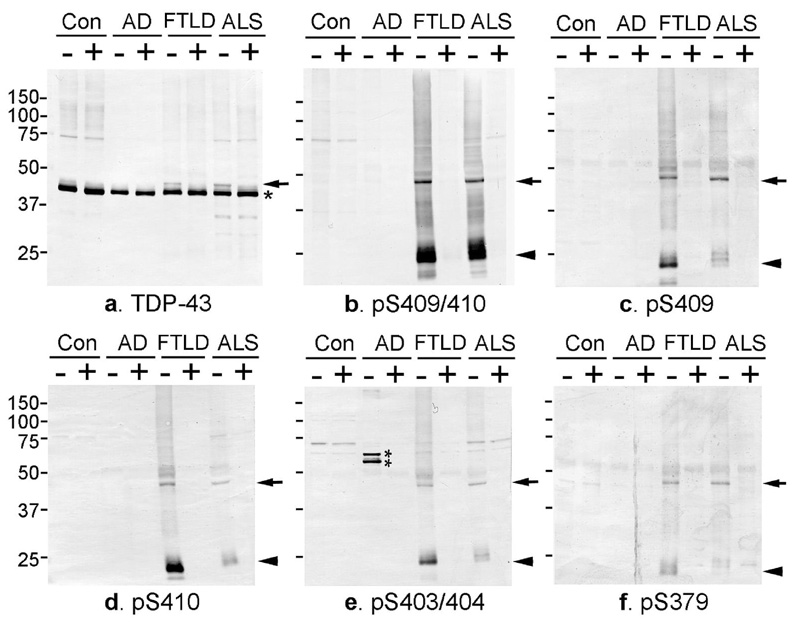
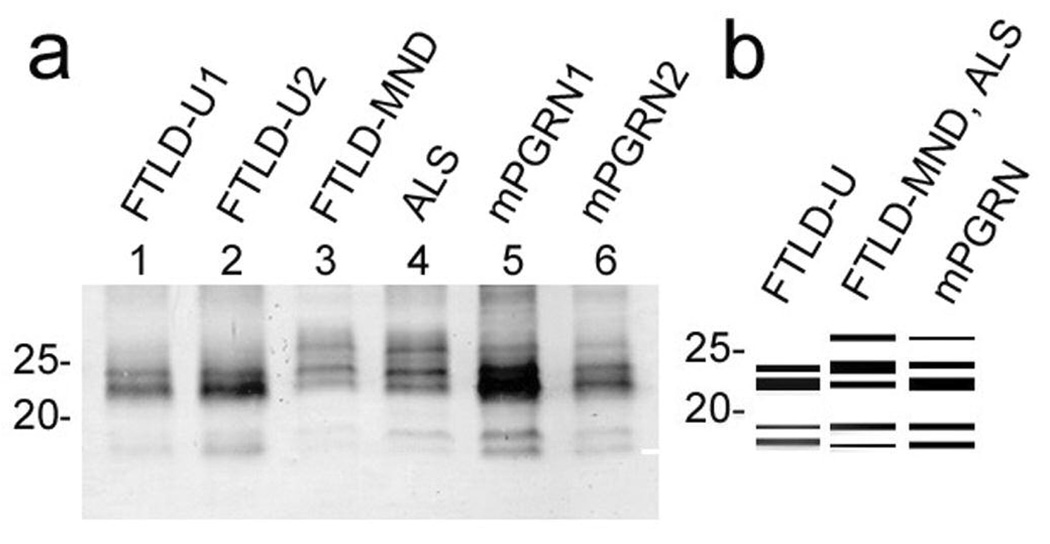
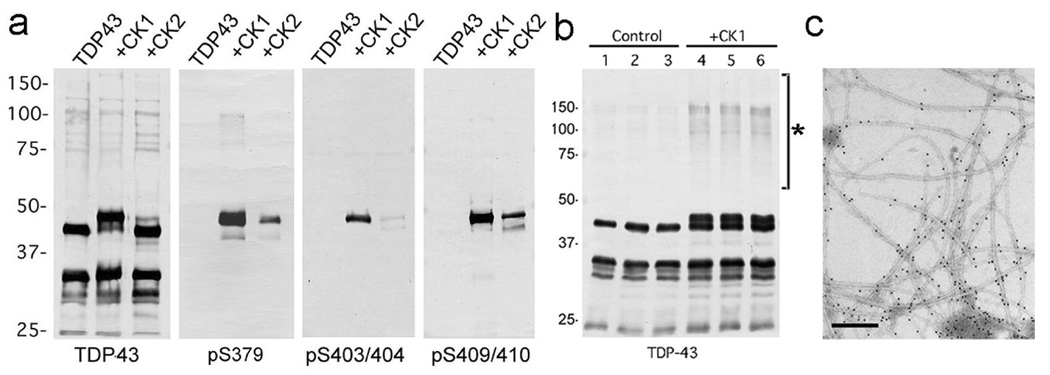
Results: We identified multiple phosphorylation sites in carboxyl-terminal regions of deposited TDP-43. Phosphorylation-specific antibodies stained more inclusions than antibodies to ubiquitin and, unlike existing commercially available anti-TDP-43 antibodies, did not stain normal nuclei. Ultrastructurally, these antibodies labeled abnormal fibers of 15nm diameter and on immunoblots recognized hyperphosphorylated TDP-43 at 45kDa, with additional 18 to 26kDa fragments in sarkosyl-insoluble fractions from FTLD-U and ALS brains. The phosphorylated epitopes were generated by casein kinase-1 and -2, and phosphorylation led to increased oligomerization and fibrillization of TDP-43.
Interpretation: These results suggest that phosphorylated TDP-43 is a major component of the inclusions, and that abnormal phosphorylation of TDP-43 is a critical step in the pathogenesis of FTLD-U and ALS. Phosphorylation-specific antibodies will be powerful tools for the investigation of these disorders.
Figures
References
-
- Mackenzie IRA, Feldman HH. Ubiquitin immunohistochemistry suggests classic motor neuron disease, motor neuron disease with dementia, and frontotemporal dementia of the motor neuron disease type represent a clinicopathological spectrum. J Neuropathol Exp Neurol. 2005;64:730–739. - PubMed
-
- Baker M, Mackenzie IR, Pickering-Brown SM, et al. Mutations in progranulin cause tau-negative frontotemporal dementia linked to chromosome 17. Nature. 2006;442:916–919. - PubMed
-
- Cruts M, Gijselinck I, van der Zee J, et al. Null mutations in progranulin cause ubiquitin-positive frontotemporal dementia linked to chromosome 17q21. Nature. 2006;442:920–924. - PubMed
-
- Watts GDJ, Wymer J, Kovach MJ, et al. Inclusion body myopathy associated with Paget disease of bone and frontotemporal dementia is caused by mutant valosin-containing protein. Nat Genet. 2004;36:377–381. - PubMed
-
- Morita M, Al-Chalabi A, Anderson PM, et al. A locus on chromosome 9p confers susceptibility to ALS and frontotemporal dementia. Neurology. 2006;66:839–844. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
