

The role of arousal related brainstem reflexes in causing recovery from upper airway occlusion in infants
- PMID: 18548828
- PMCID: PMC2442409
- DOI: 10.1093/sleep/31.6.833
The role of arousal related brainstem reflexes in causing recovery from upper airway occlusion in infants
Abstract
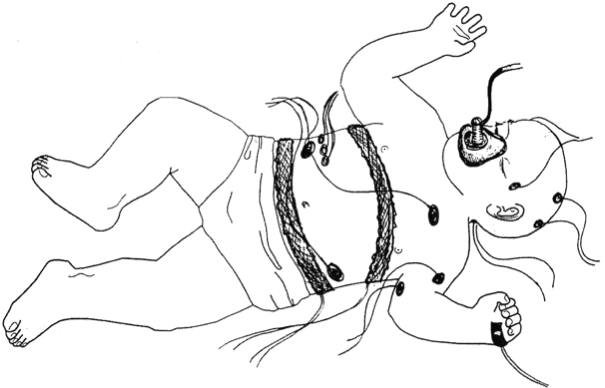
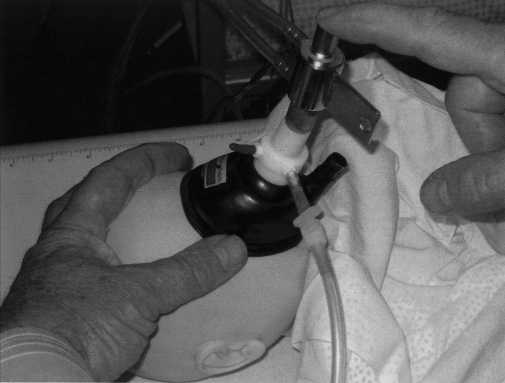
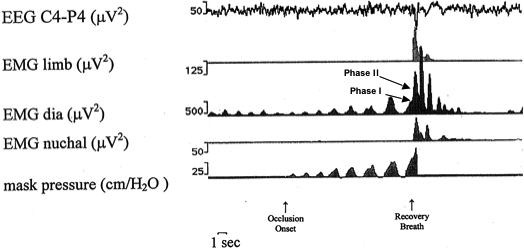
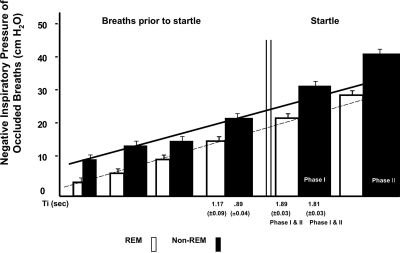
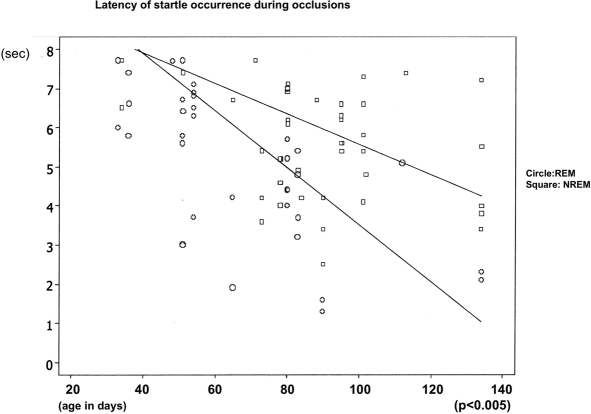
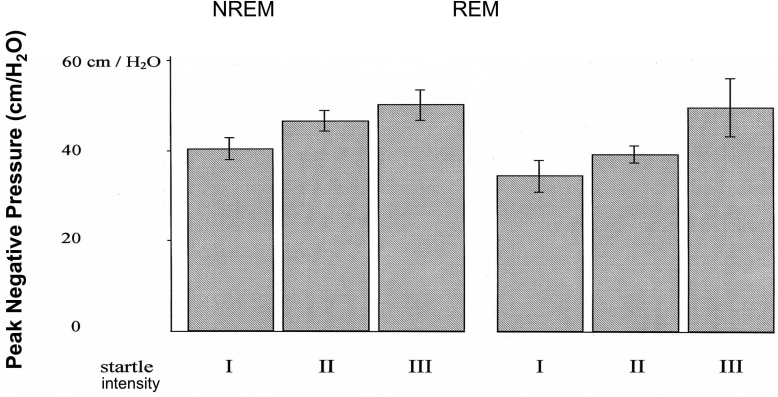
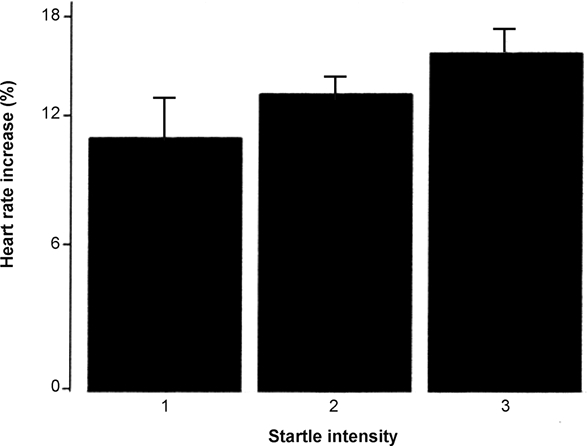
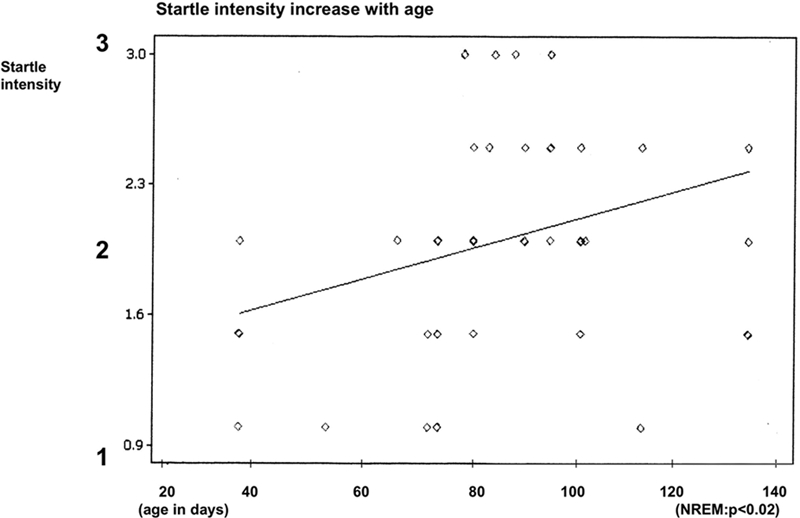
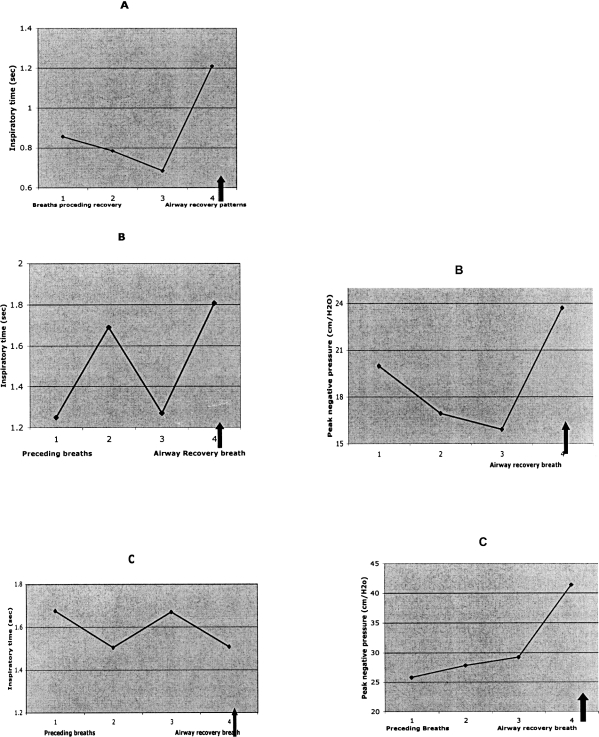
During obstructive sleep apnea (OSA) in adults upper airway reopening coincides with a sudden burst in activity of pharyngeal dilating muscles. This has been attributed to arousal from sleep as indicated by increased EEG activity. Recovery from OSA in infants often occurs in the absence of cortical arousal. To investigate mechanisms involved in recovery, we performed experimental airway occlusions in sleeping infants. Based on past work, our hypothesis was that a sleep startle combined with an augmented breath and heart rate acceleration would occur during the occlusion, and that such brainstem mediated reflexes might provide an explanation for recovery from OSA in the absence of cortical arousal. However, this is contrary to expectations, since lung inflation is believed to be necessary for occurrence of an augmented breath. We studied 16 healthy infants during sleep. We recorded EEG, EOG, ECG, oxygen saturation, diaphragmatic, nuchal and limb electromyograms, face mask pressure, and airflow. A startle, accompanied by neck extension, limb and nuchal EMG activation, as well as heart rate acceleration occurred during all airway occlusions. The startle occurred simultaneously with a large biphasic inspiratory effort, having characteristics of an augmented breath (sigh). In more than a third of cases, this occurred without any evidence of cortical arousal activity. The magnitude of startles as well as the increase in heart rate correlated positively with peak airway negative pressure, indicating that arousal processes are graded in intensity. We conclude that the neck extension and pharyngeal dilating muscle activity associated with the startle and augmented breath may account for recovery of airway patency in infants as they do adults. Lung inflation is not a prerequisite for the reflex to occur.
Figures
References
-
- Anders T, Emde R, Parmalee A. UCLA Brain Information Service. Los Angeles: BRI Publications Office; 1971. A manual of standardized terminology, technology, and criteria for scoring of states of sleep and wakefulness in newborn infants.
-
- Bartlett D. Origin and regulation of spontaneous deep breaths. Respir Physiol. 1971;12:230–8. - PubMed
-
- Berry RB, Gleeson K. Respiratory arousal from sleep: mechanisms and significance. Sleep. 1997;20:654–75. - PubMed
-
- Brouillette RT, Thach BT. Control of genioglossus muscle inspiratory activity. J Appl Physiol. 1980;49:801–8. - PubMed
-
- Davis, M . The mammalian startle response. In: Eaton RC, editor. Neural mechanisms of startle behavior. New York: Plenum Press; 1984.
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
