

Management of obscure occult gastrointestinal bleeding: a cost-minimization analysis
- PMID: 18550005
- PMCID: PMC2652579
- DOI: 10.1016/j.cgh.2008.02.033
Management of obscure occult gastrointestinal bleeding: a cost-minimization analysis
Abstract
Background & aims: Capsule endoscopy (CE) and double-balloon enteroscopy (DBE) allow complete small-bowel examination but consume additional health care resources. A cost-minimization analysis determined the optimal initial management strategy for obscure occult gastrointestinal bleeding (OGIB).
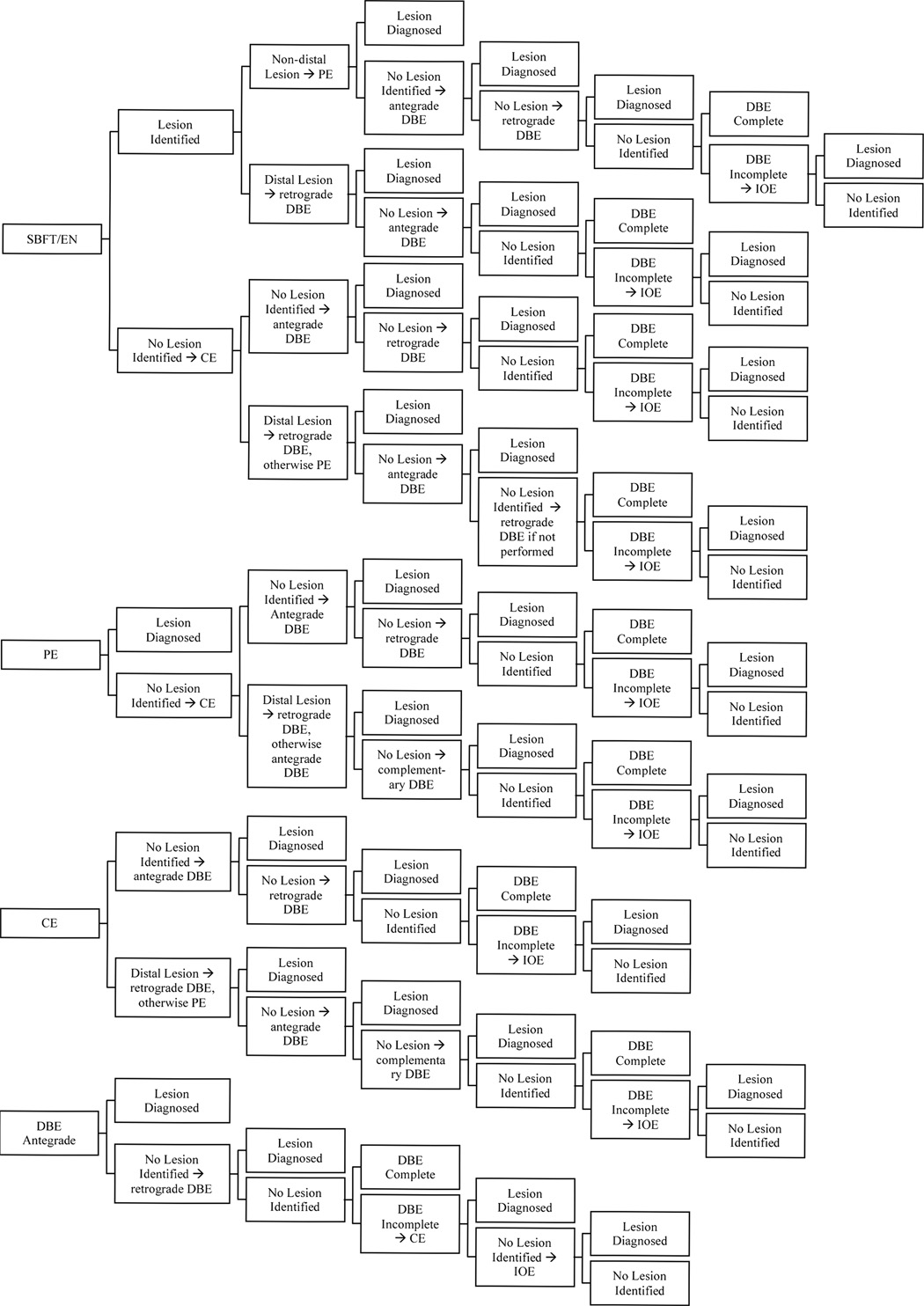
Methods: We compared 5 strategies: initial small-bowel follow-through, enteroclysis, push enteroscopy (PE), CE, or DBE. Incorporation of multiple tests was allowed with costs taken from a third-party payer perspective. We modeled medically refractory disease with 2 separate model end points in which treatment or definitive diagnosis was necessary and in which visual diagnosis was sufficient to suspend testing. Sensitivity analyses included variations in parameter estimates, Monte Carlo simulation, and structural variations in the model in which DBE was not available as an initial strategy.
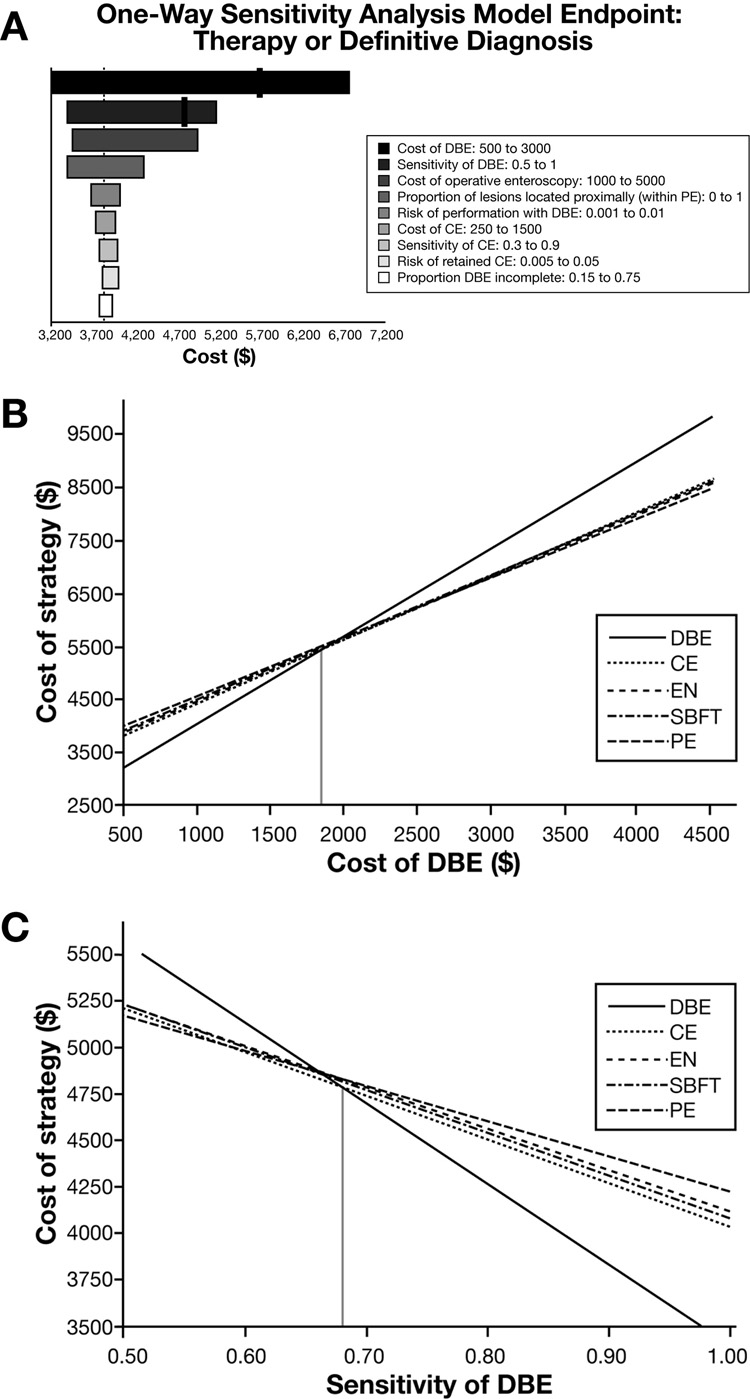
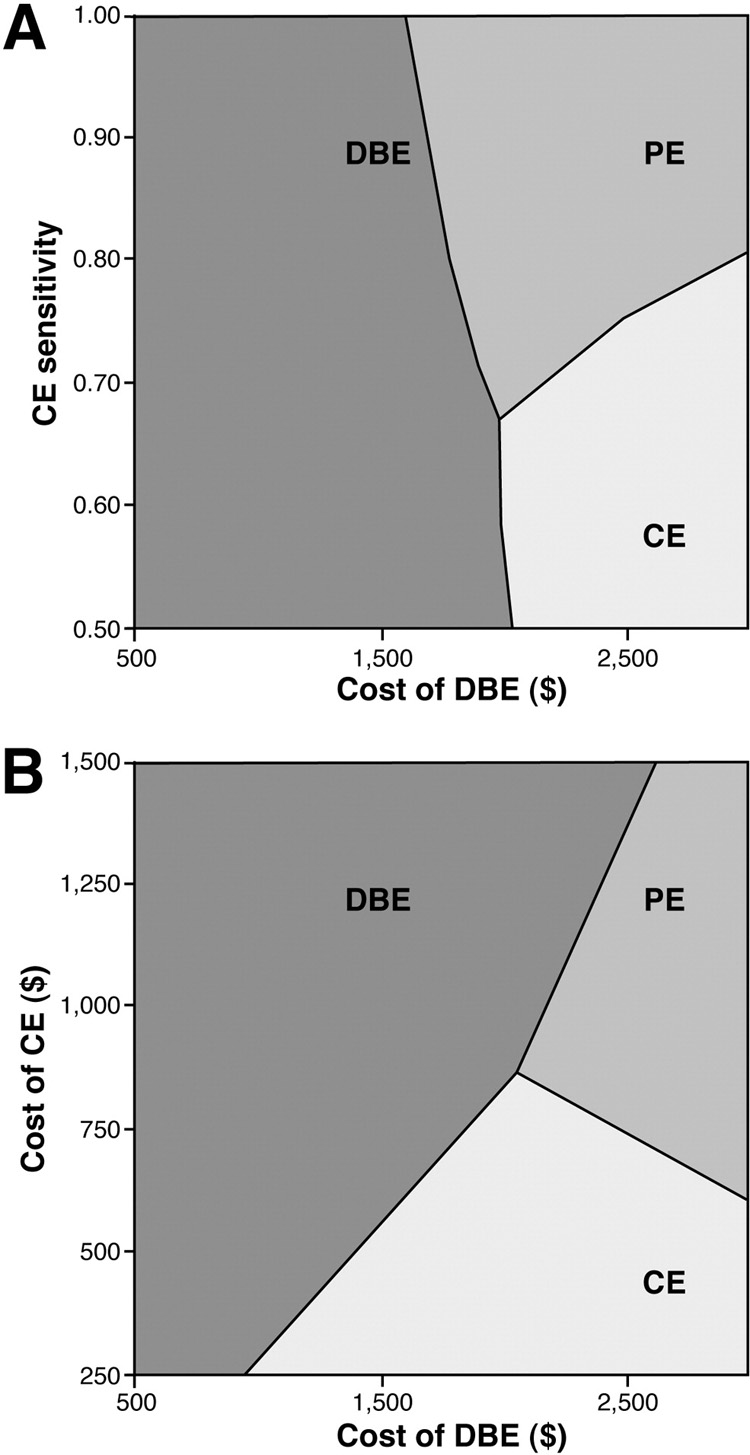
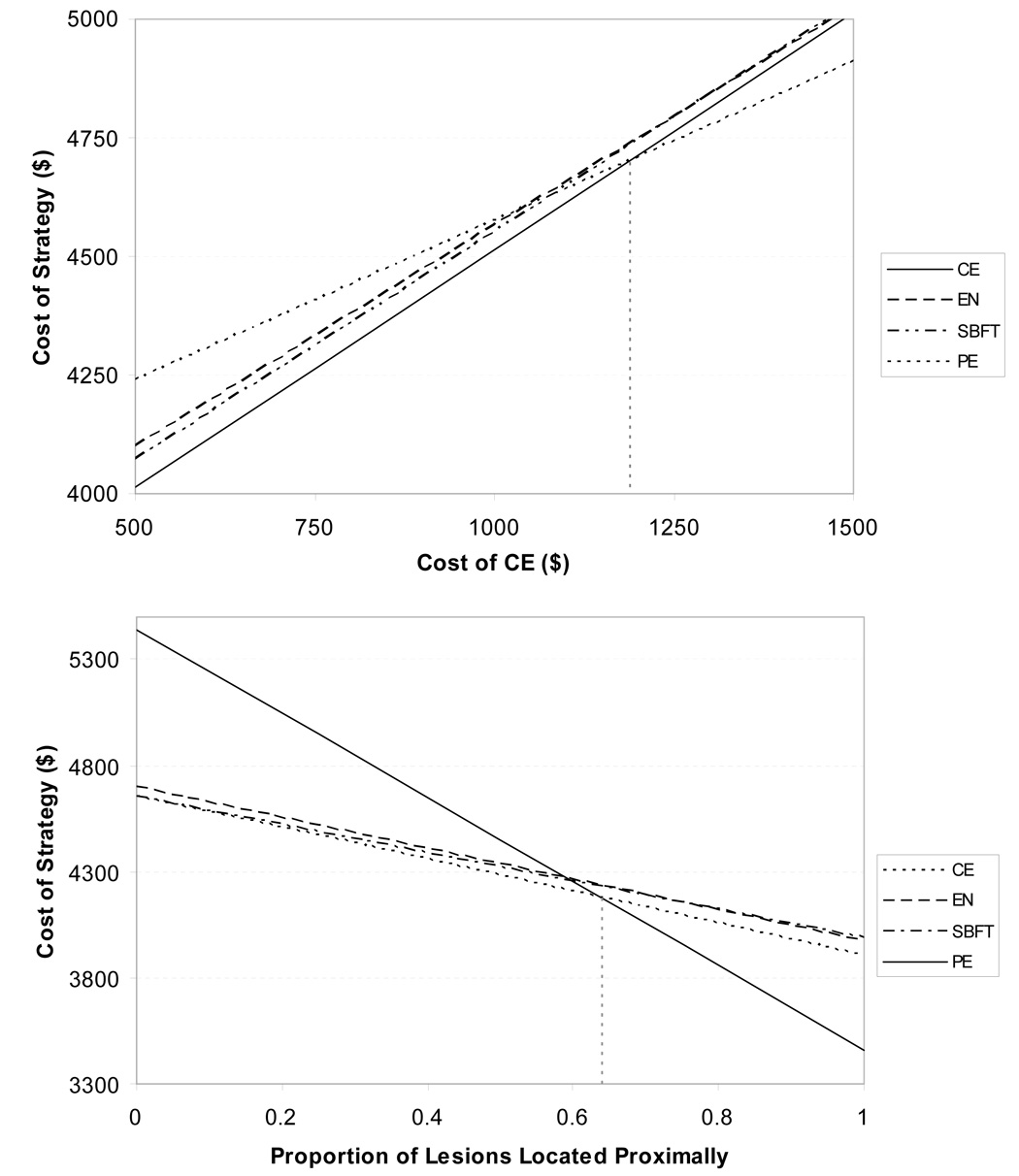
Results: When treatment or definitive diagnosis was necessary, the optimal strategy was initial DBE at a cost of $3824. An initial CE strategy costs an incremental $440. CE was preferred when DBE exceeded $1849 or when the sensitivity of DBE decreased to less than 68%. If DBE was unavailable as an initial test then CE was preferred to PE unless CE exceeded $1190, capsule retention was greater than 3%, or 64% of lesions were within reach of PE. When visual diagnosis was sufficient, initial CE was preferred.
Conclusions: For OGIB, initial DBE may be the least expensive strategy when treatment or definitive diagnosis is necessary and initial CE may be preferred when visual identification is sufficient. In settings where DBE is not available as an initial test, initial CE may be the preferred strategy.
Figures
References
-
- Zuckerman GR, Prakash C, Askin MP, Lewis BS. AGA technical review on the evaluation and management of occult and obscure gastrointestinal bleeding. Gastroenterology. 2000;118:201–221. - PubMed
-
- Heine GD, Hadithi M, Groenen MJ, Kuipers EJ, Jacobs MA, Mulder CJ. Double-balloon enteroscopy: indications, diagnostic yield, and complications in a series of 275 patients with suspected small-bowel disease. Endoscopy. 2006;38:42–48. - PubMed
-
- Prakash C, Zuckerman GR. Acute small bowel bleeding: a distinct entity with significantly different economic implications compared with GI bleeding from other locations. Gastrointest Endosc. 2003;58:330–335. - PubMed
-
- Lewis BS. Small intestinal bleeding. Gastroenterol Clin North Am. 1994;23:67–91. - PubMed
-
- Lewis B, Goldfarb N. Review article: The advent of capsule endoscopy--a not-so-futuristic approach to obscure gastrointestinal bleeding. Aliment Pharmacol Ther. 2003;17:1085–1096. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
