

A prognostic model for one-year mortality in patients requiring prolonged mechanical ventilation
- PMID: 18552692
- PMCID: PMC2728216
- DOI: 10.1097/CCM.0b013e31817b8925
A prognostic model for one-year mortality in patients requiring prolonged mechanical ventilation
Abstract
Objective: A measure that identifies patients who are at high risk of mortality after prolonged ventilation will help physicians communicate prognoses to patients or surrogate decision makers. Our objective was to develop and validate a prognostic model for 1-yr mortality in patients ventilated for 21 days or more.
Design: The authors conducted a prospective cohort study.
Setting: The study took place at a university-based tertiary care hospital.
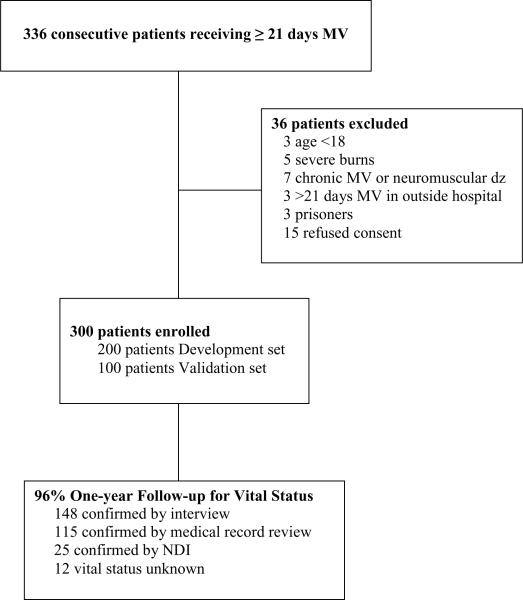
Patients: Three hundred consecutive medical, surgical, and trauma patients requiring mechanical ventilation for at least 21 days were prospectively enrolled.
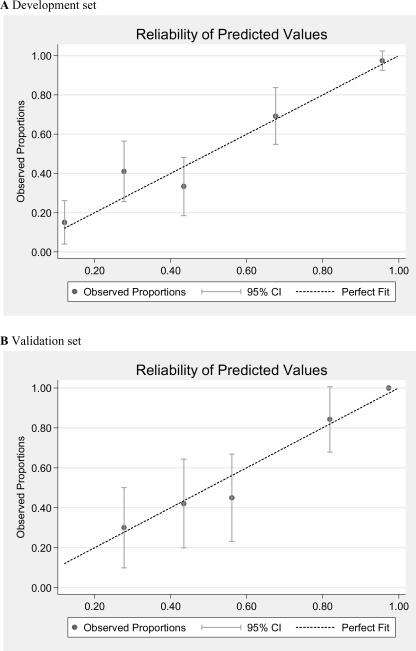
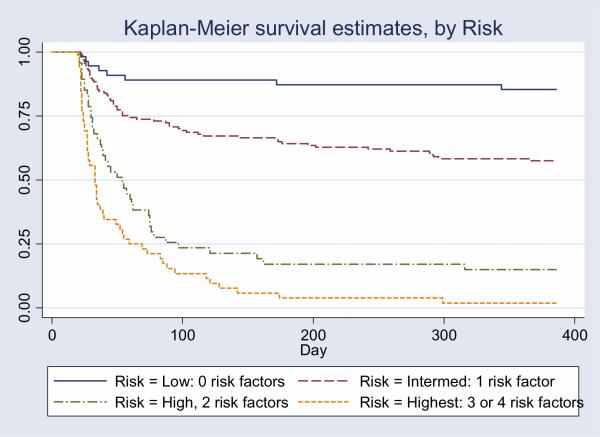
Measurements and main results: Predictive variables were measured on day 21 of ventilation for the first 200 patients and entered into logistic regression models with 1-yr and 3-mo mortality as outcomes. Final models were validated using data from 100 subsequent patients. One-year mortality was 51% in the development set and 58% in the validation set. Independent predictors of mortality included requirement for vasopressors, hemodialysis, platelet count < or = 150 x 10(9)/L, and age > or = 50 yrs. Areas under the receiver operating characteristic curve for the development model and validation model were .82 (SE .03) and .82 (SE .05), respectively. The model had sensitivity of .42 (SE .12) and specificity of .99 (SE .01) for identifying patients who had > or = 90% risk of death at 1 yr. Observed mortality was highly consistent with both 3- and 12-mo predicted mortality. These four predictive variables can be used in a simple prognostic score that clearly identifies low-risk patients (no risk factors, 15% mortality) and high-risk patients (three or four risk factors, 97% mortality).
Conclusions: Simple clinical variables measured on day 21 of mechanical ventilation can identify patients at highest and lowest risk of death from prolonged ventilation.
Figures
Comment in
-
Objective rather than subjective evaluation of prognosis in patients on prolonged mechanical ventilation: the ProVent score.Crit Care Med. 2008 Jul;36(7):2200-1. doi: 10.1097/CCM.0b013e31817d7d5e. Crit Care Med. 2008. PMID: 18594231 No abstract available.
References
-
- MacIntyre NR, Epstein SK, Carson S, Scheinhorn S, Christopher K, Muldoon S. Management of patients requiring prolonged mechanical ventilation: report of a NAMDRC consensus conference. Chest. 2005;128(6):3937–3954. - PubMed
-
- Carson SS, Bach PB. The epidemiology and costs of chronic critical illness. Crit Care Clin. 2002;18(3):461–76. - PubMed
-
- Cox CE, Carson SS, Holmes GM, Howard A, Carey TS. Increase in tracheostomy for prolonged mechanical ventilation in North Carolina, 1993-2002. Crit Care Med. 2004;32(11):2219–26. - PubMed
-
- Wagner DP. Economics of prolonged mechanical ventilation. Am Rev Respir Dis. 1989;140(2 Pt 2):S14–8. - PubMed
-
- Douglas SL, Daly BJ, Gordon N, Brennan PF. Survival and quality of life: short-term versus long-term ventilator patients. Crit Care Med. 2002;30(12):2655–62. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
