

Smoke inhalation lung injury: an update
- PMID: 18552974
- PMCID: PMC2396464
Smoke inhalation lung injury: an update
Abstract
Objectives: The purpose of this study is to present a multifaceted, definitive review of the past and current status of smoke inhalation injury. History along with current understanding of anatomical, physiology, and biologic components will be discussed.
Methods: The literature has been reviewed from the early onset of the concept of smoke inhalation in the 1920s to our current understanding as of 2007.
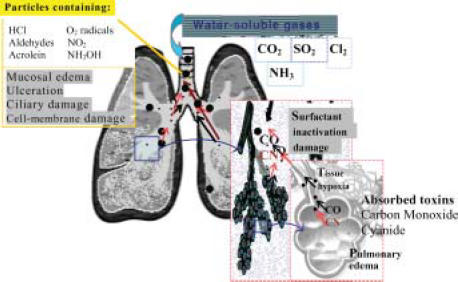
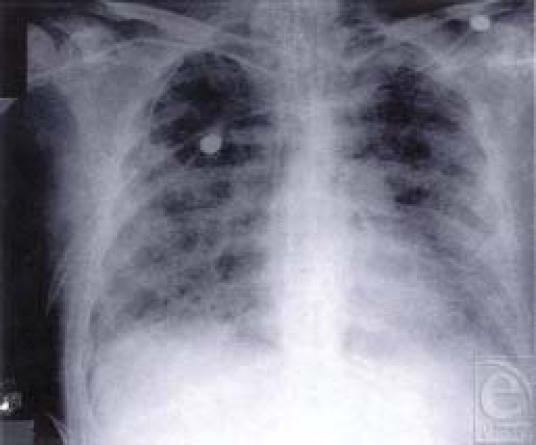
Results: The results indicate that the current pathophysiologic concept is of a disease process that leads to immediate and delayed pulmonary injury best managed by aggressive physiologic support. Management approaches for the biochemical changes have not kept up with current knowledge. The lung injury process is activated by toxins in the smoke's gas and particle components and perpetuated by a resulting lung inflammation. This inflammatory process becomes self-perpetuating through the activation of a large number of inflammatory cascades. In addition, smoke injury leads to significant systemic abnormalities injuring other organs and accentuating the burn injury process and subsequently leading to mediator-induced cellular injury leading potentially to multisystem organ failure.
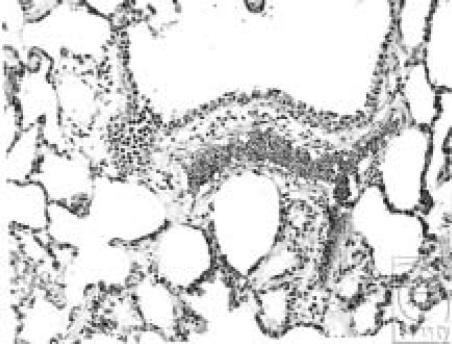
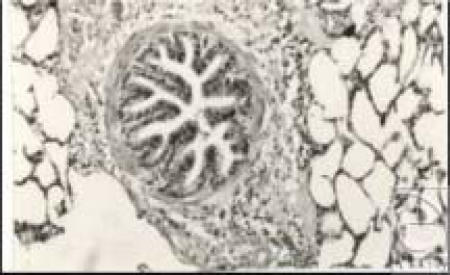
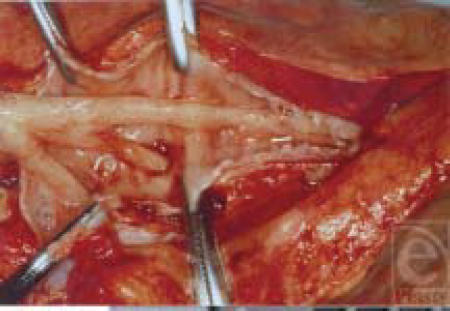
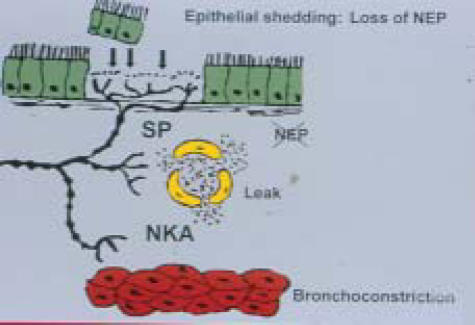
Conclusions: Smoke inhalation injury results in the anatomic finding of denuded and sometimes sloughed airways mucosa. Physiologic findings include small airways containing fibrin casts of mucosa and neutrophils. Airway hyper-reactivity results as well, leading to further decreased collapse, causing obstruction.
Figures




References
-
- Traber D, Pollard V. Pathophysiology of Inhalation Injury. In: Herndon D, editor. Total Burn Care. Philadelphia Pa: Saunders; 2002. 175 pp.
-
- Sachor F, Amllory G. Lung lesions in patients dying of burns. Arch Pathol. 1963;75:303–8. - PubMed
-
- Thompson P, Herndon D, et al. Effect on mortality of inhalation injury. Trauma. 1986;26:163–5. - PubMed
-
- Winternatz MC. Pathology of War Gas Poisoning. Princeton, NJ: Yale University Press; 1920.
LinkOut - more resources
Full Text Sources
Miscellaneous