

Prognostic value of perfusion MR imaging of high-grade astrocytomas: long-term follow-up study
- PMID: 18556364
- PMCID: PMC8119049
- DOI: 10.3174/ajnr.A1121
Prognostic value of perfusion MR imaging of high-grade astrocytomas: long-term follow-up study
Abstract
Background and purpose: Although the prognostic value of perfusion MR imaging in various gliomas has been investigated, that in high-grade astrocytomas alone has not been fully evaluated. The purpose of this study was to evaluate retrospectively whether the tumor maximum relative cerebral blood volume (rCBV) on pretreatment perfusion MR imaging is of prognostic value in patients with high-grade astrocytoma.
Materials and methods: Between January 1999 and December 2002, 49 patients (30 men, 19 women; age range, 23-76 years) with supratentorial high-grade astrocytoma underwent MR imaging before the inception of treatment. The patient age, sex, symptom duration, neurologic function, mental status, Karnofsky Performance Scale, extent of surgery, histopathologic diagnosis, tumor component enhancement, and maximum rCBV were assessed to identify factors affecting survival. Kaplan-Meier survival curves, the logrank test, and the multivariate Cox proportional hazards model were used to evaluate prognostic factors.
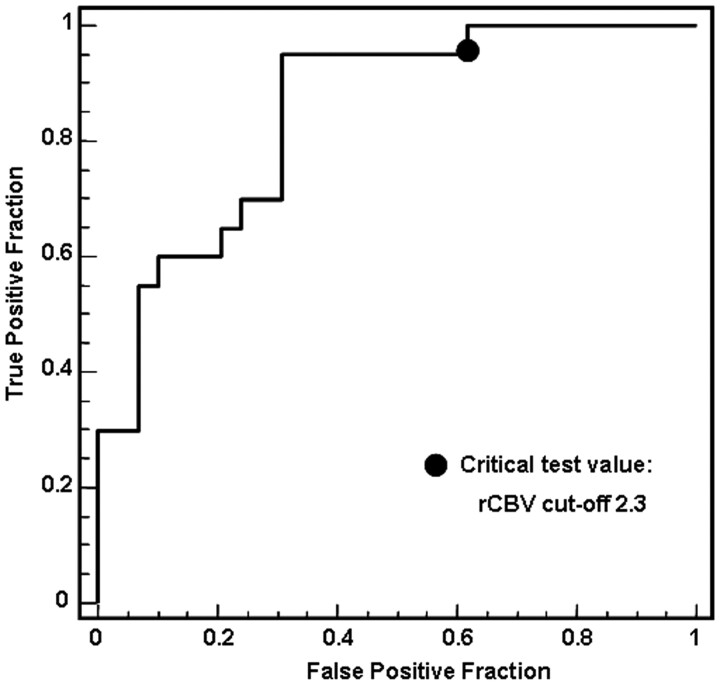
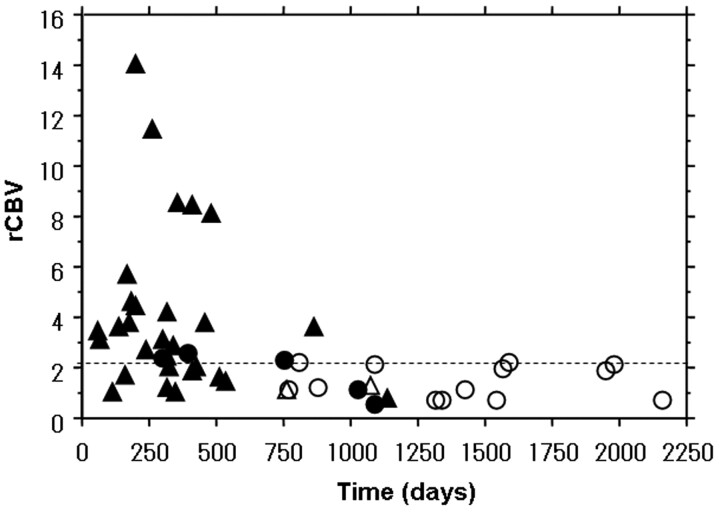
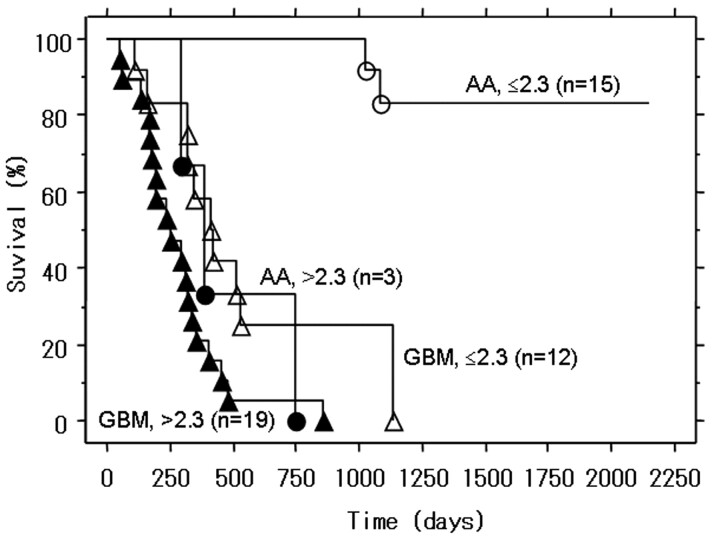
Results: The maximum rCBV was significantly higher in the 31 patients with glioblastoma multiforme than in the 18 with anaplastic astrocytoma (P < .03). The 2-year overall survival rate was 67% for 27 patients with a low (< or =2.3) and 9% for 22 patients with a high (>2.3) maximum rCBV value (P < .001). Independent important prognostic factors were the histologic diagnosis (hazard ratio = 9.707; 95% confidence interval (CI), 3.163-29.788), maximum rCBV (4.739; 95% CI, 1.950-11.518), extent of surgery (2.692; 95% CI, 1.196-6.061), and sex (2.632; 95% CI, 1.153-6.010).
Conclusion: The maximum rCBV at pretreatment perfusion MR imaging is a useful clinical prognostic biomarker for survival in patients with high-grade astrocytoma.
Figures
References
-
- Louis DN, Ohgaki H, Wiestler OD, et al. World Health Organization Classification of Tumours of the Central Nervous System: Astrocytic Tumours. Lyon, France: IARC Press;2007. :13–52
-
- Gupta T, Sarin R. Poor-prognosis high-grade gliomas: evolving an evidence-based standard of care. Lancet Oncol 2002;3:557–64 - PubMed
-
- Behin A, Hoang-Xuan K, Carpentier AF, et al. Primary brain tumours in adults. Lancet 2003;361:323–31 - PubMed
-
- Stewart LA. Chemotherapy in adult high-grade glioma: a systematic review and meta-analysis of individual patient data from 12 randomised trials. Lancet 2002;359:1011–18 - PubMed
-
- Scott CB, Scarantino C, Urtasun R, et al. Validation and predictive power of Radiation Therapy Oncology Group (RTOG) recursive partitioning analysis classes for malignant glioma patients: a report using RTOG 90–06. Int J Radiat Oncol Biol Phys 1998;40:51–55 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical