

Local activation or implantation of cardiac progenitor cells rescues scarred infarcted myocardium improving cardiac function
- PMID: 18556576
- PMCID: PMC2747796
- DOI: 10.1161/CIRCRESAHA.108.178525
Local activation or implantation of cardiac progenitor cells rescues scarred infarcted myocardium improving cardiac function
Abstract
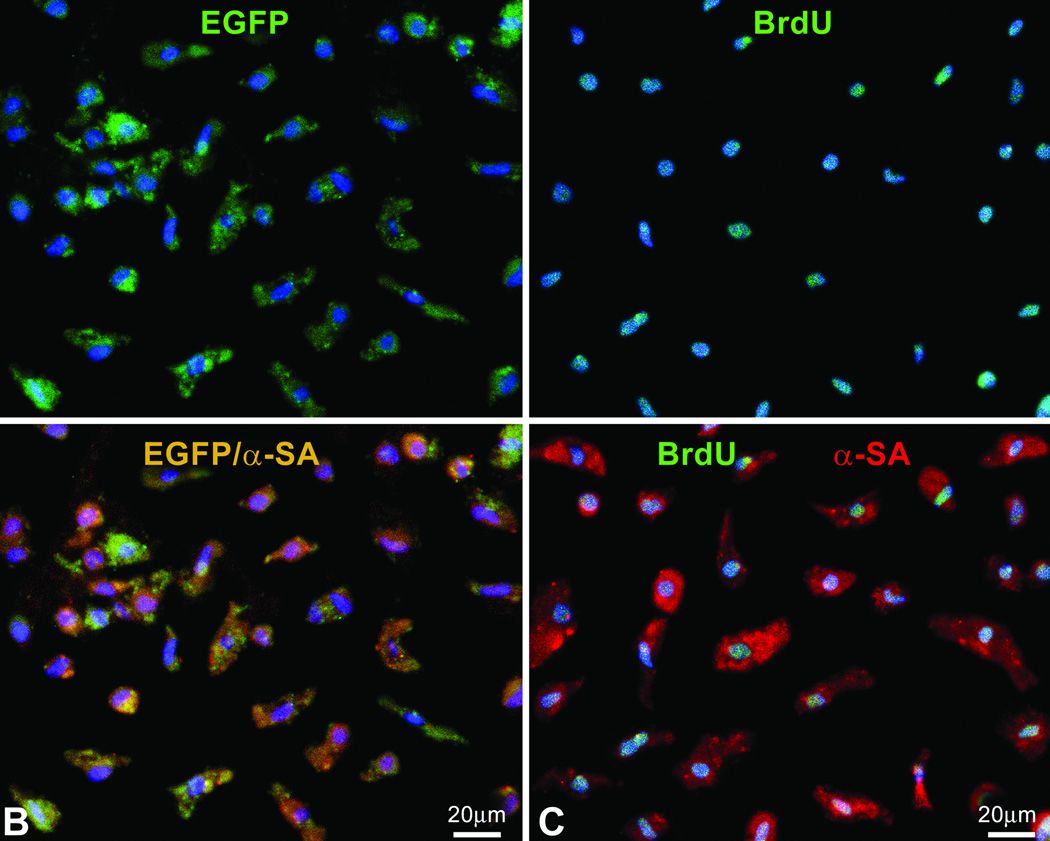
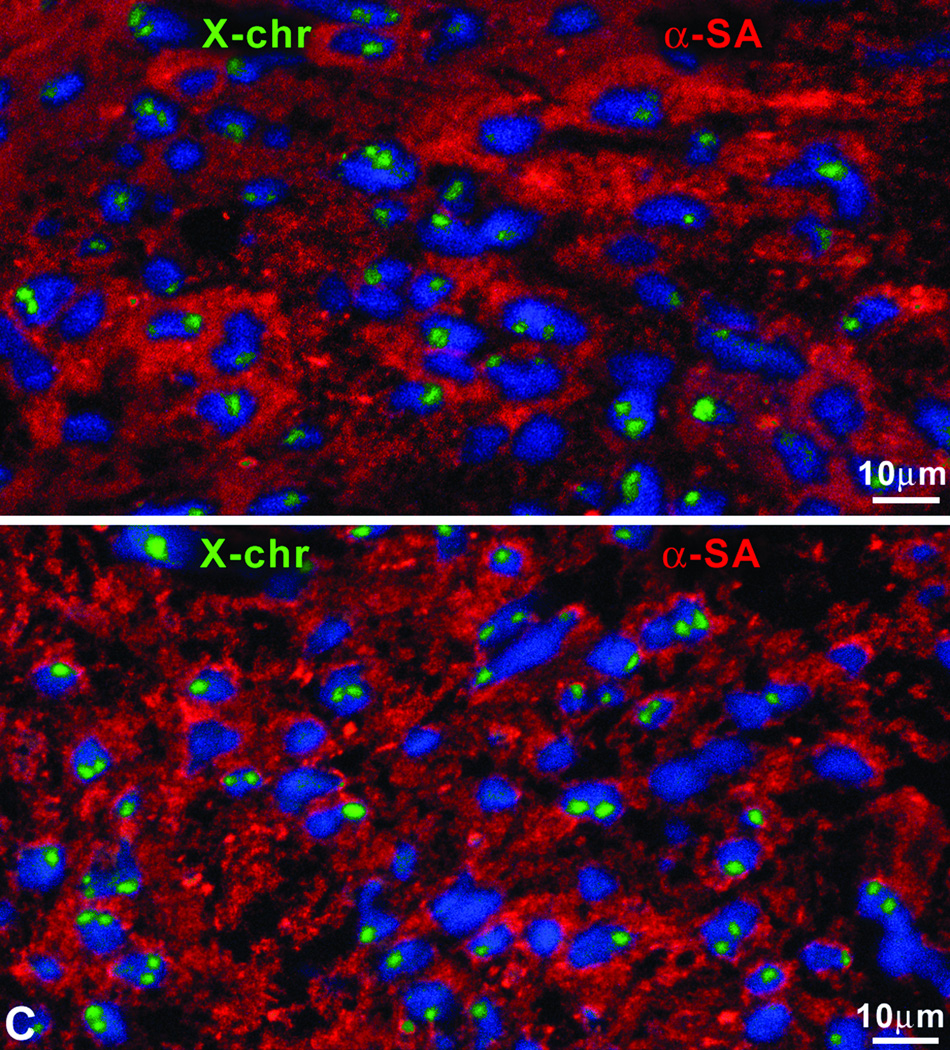
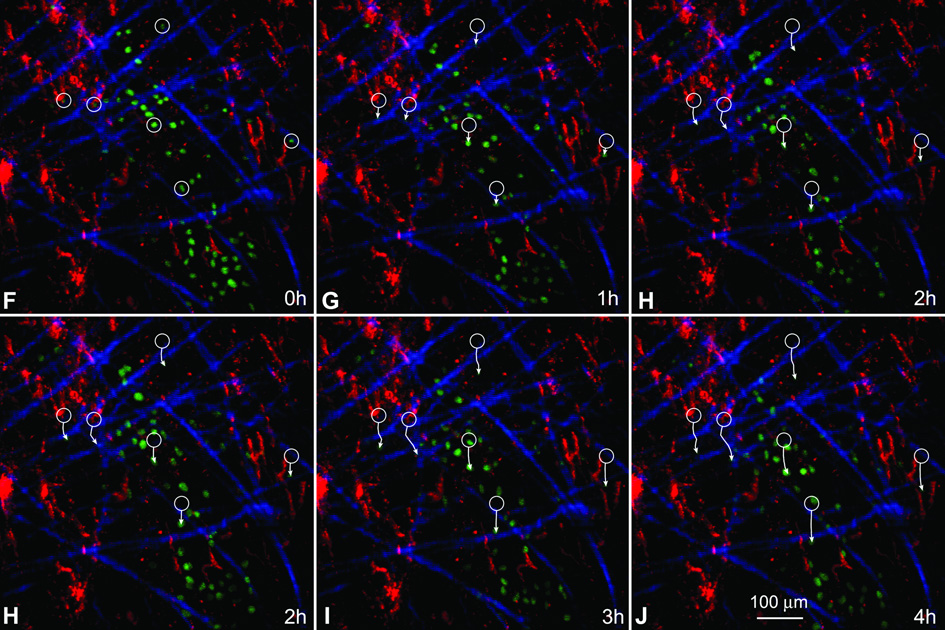
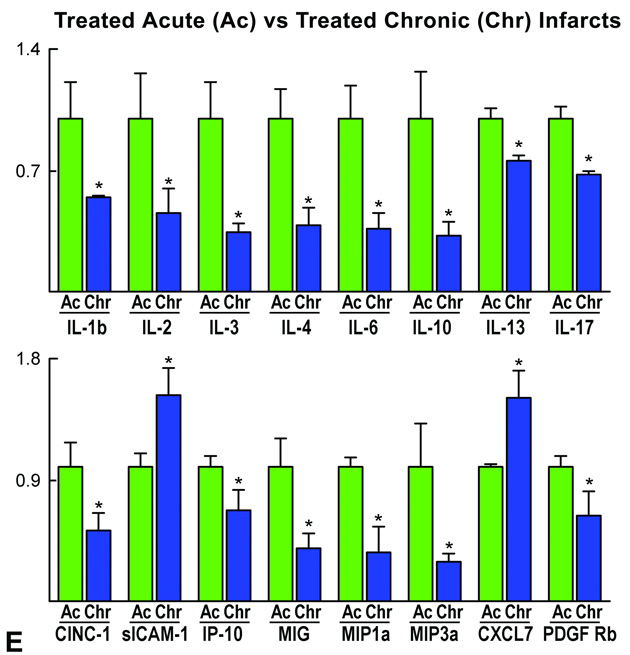
Ischemic heart disease is characterized chronically by a healed infarct, foci of myocardial scarring, cavitary dilation, and impaired ventricular performance. These alterations can only be reversed by replacement of scarred tissue with functionally competent myocardium. We tested whether cardiac progenitor cells (CPCs) implanted in proximity of healed infarcts or resident CPCs stimulated locally by hepatocyte growth factor and insulin-like growth factor-1 invade the scarred myocardium and generate myocytes and coronary vessels improving the hemodynamics of the infarcted heart. Hepatocyte growth factor is a powerful chemoattractant of CPCs, and insulin-like growth factor-1 promotes their proliferation and survival. Injection of CPCs or growth factors led to the replacement of approximately 42% of the scar with newly formed myocardium, attenuated ventricular dilation and prevented the chronic decline in function of the infarcted heart. Cardiac repair was mediated by the ability of CPCs to synthesize matrix metalloproteinases that degraded collagen proteins, forming tunnels within the fibrotic tissue during their migration across the scarred myocardium. New myocytes had a 2n karyotype and possessed 2 sex chromosomes, excluding cell fusion. Clinically, CPCs represent an ideal candidate cell for cardiac repair in patients with chronic heart failure. CPCs may be isolated from myocardial biopsies and, following their expansion in vitro, administered back to the same patients avoiding the adverse effects associated with the use of nonautologous cells. Alternatively, growth factors may be delivered locally to stimulate resident CPCs and promote myocardial regeneration. These forms of treatments could be repeated over time to reduce progressively tissue scarring and expand the working myocardium.
Figures















References
-
- Leri A, Kajstura J, Anversa P. Cardiac stem cells and mechanisms of myocardial regeneration. Physiol Rev. 2005;85:1373–1416. - PubMed
-
- Urbanek K, Torella D, Sheikh F, De Angelis A, Nurzynska D, Silvestri F, Beltrami CA, Bussani R, Beltrami AP, Quaini F, Bolli R, Leri A, Kajstura J, Anversa P. Myocardial regeneration by activation of multipotent cardiac stem cells in ischemic heart failure. Proc Natl Acad Sci USA. 2005;102:8692–8697. - PMC - PubMed
-
- Beltrami AP, Urbanek K, Kajstura J, Yan SM, Finato N, Bussani R, Nadal-Ginard B, Silvestri F, Leri A, Beltrami CA, Anversa P. Evidence that human cardiac myocytes divide after myocardial infarction. New Engl J Med. 2001;334:1750–1757. - PubMed
-
- Beltrami AP, Barlucchi L, Torella D, Baker M, Chimenti S, Kasahara H, Rota M, Musso E, Urbanek K, Leri A, Kajstura J, Nadal-Ginard B, Anversa P. Adult cardiac stem cells are multipotent and support myocardial regeneration. Cell. 2003;114:763–766. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
