

Single daily dosing ceftriaxone and metronidazole vs standard triple antibiotic regimen for perforated appendicitis in children: a prospective randomized trial
- PMID: 18558169
- PMCID: PMC3082440
- DOI: 10.1016/j.jpedsurg.2008.02.018
Single daily dosing ceftriaxone and metronidazole vs standard triple antibiotic regimen for perforated appendicitis in children: a prospective randomized trial
Abstract
Introduction: Appendicitis is the most common emergency condition in children. Historically, a 3-drug regimen consisting of ampicillin, gentamicin, and clindamycin (AGC) has been used postoperatively for perforated appendicitis. A retrospective review at our institution has found single day dosing of ceftriaxone and metronidazole (CM) to be a more simple and cost-effective antibiotic strategy. Therefore, we performed a prospective, randomized trial to compare efficacy and cost-effectiveness of these 2 regimens.
Methods: After internal review board approval (IRB no. 04 12-149), children found to have perforated appendicitis at appendectomy were randomized to either once daily dosing of CM (2 total doses per day) or standard dosing of AGC (11 total doses per day). Perforation was defined as an identifiable hole in the appendix. The operative approach (laparoscopic), length of antibiotic use, and criteria for discharge were standardized for the groups. Based on our retrospective analysis using length of postoperative hospitalization as a primary end point, a sample size of 100 patients was calculated for an alpha of .5 and a power of 0.82.
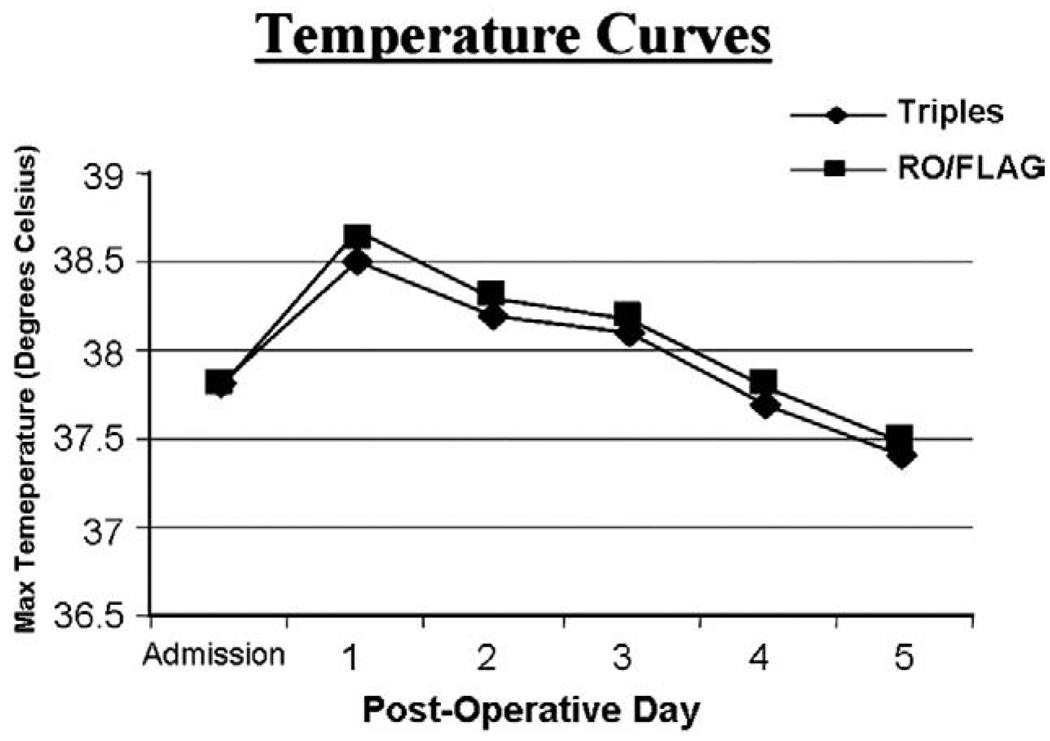
Results: One hundred patients underwent laparoscopic appendectomy for perforated appendicitis. On presentation, there were no differences in sex distribution, days of symptoms, temperature, or leukocyte count. There was no difference in abscess rate or wound infections between groups. The CM group resulted in significantly less antibiotic charges then the AGC group.
Conclusions: Once daily dosing with the 2-drug regimen (CM) offers a more efficient, cost-effective antibiotic management in children with perforated appendicitis without compromising infection control when compared to a traditional 3-drug regimen.
Figures
Comment in
-
Considerations about the article by St. Peter "Single daily dosing ceftriaxone and metronidazole vs standard triple antibiotic regimen for perforated appendicitis in children: a prospective randomised trial". J Pediatr Surg 2008;43:981-985.J Pediatr Surg. 2008 Oct;43(10):1949; author reply 1949-50. doi: 10.1016/j.jpedsurg.2008.07.023. J Pediatr Surg. 2008. PMID: 18926241 No abstract available.
References
-
- St Peter SD, Little DC, Calkins CM, et al. A simple and more cost-effective antibiotic regimen for perforated appendicitis. J Pediatr Surg. 2006;41:1020–1024. - PubMed
-
- St. Peter SD, Little DC, Calkins CM, et al. Does routine nasogastric tube placement after an operation for perforated appendicitis make a difference. J Surg Res. 2007;143(1):66–69. - PubMed
-
- Results of the North American trial of piperacillin/tazobactam compared with clindamycin and gentamicin in the treatment of severe intra-abdominal infections. Investigators of the Piperacillin/Tazobactam Tazobactam Intra-abdominal Infection Study Group. Eur J Surg Suppl. 1994;573:61–66. - PubMed
-
- Nadler EP, Reblock KK, Ford HR, et al. Monotherapy versus multi-drug therapy for the treatment of perforated appendicitis in children. Surg Infect (Larchmt) 2003;4:327–333. - PubMed
-
- Maltezou HC, Nikolaidis P, Lebesii E, et al. Piperacillin/Tazobactam versus cefotaxime plus metronidazole for treatment of children with intra-abdominal infections requiring surgery. Eur J Clin Microbiol Infect Dis. 2001;20:643–646. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
