

Prostate cancer-specific survival following salvage radiotherapy vs observation in men with biochemical recurrence after radical prostatectomy
- PMID: 18560003
- PMCID: PMC3076799
- DOI: 10.1001/jama.299.23.2760
Prostate cancer-specific survival following salvage radiotherapy vs observation in men with biochemical recurrence after radical prostatectomy
Abstract
Context: Biochemical disease recurrence after radical prostatectomy often prompts salvage radiotherapy, but no studies to date have had sufficient numbers of patients or follow-up to determine whether radiotherapy improves survival, and if so, the subgroup of men most likely to benefit.
Objectives: To quantify the relative improvement in prostate cancer-specific survival of salvage radiotherapy vs no therapy after biochemical recurrence following prostatectomy, and to identify subgroups for whom salvage treatment is most beneficial.
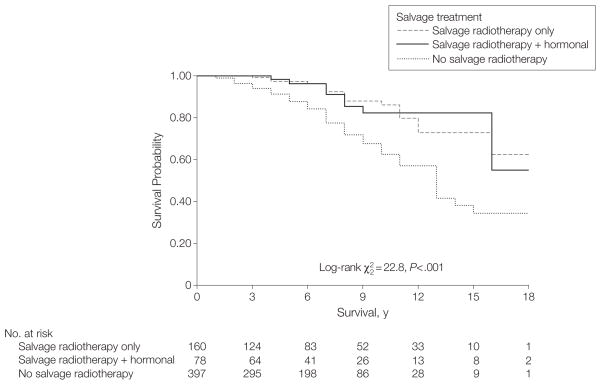
Design, setting, and patients: Retrospective analysis of a cohort of 635 US men undergoing prostatectomy from 1982-2004, followed up through December 28, 2007, who experienced biochemical and/or local recurrence and received no salvage treatment (n = 397), salvage radiotherapy alone (n = 160), or salvage radiotherapy combined with hormonal therapy (n = 78).
Main outcome measure: Prostate cancer-specific survival defined from time of recurrence until death from disease.
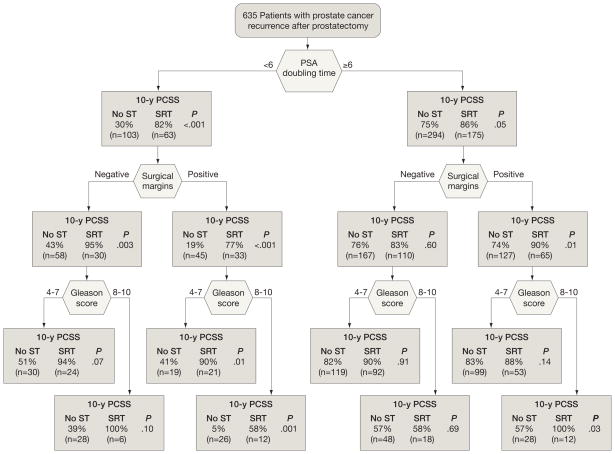
Results: With a median follow-up of 6 years after recurrence and 9 years after prostatectomy, 116 men (18%) died from prostate cancer, including 89 (22%) who received no salvage treatment, 18 (11%) who received salvage radiotherapy alone, and 9 (12%) who received salvage radiotherapy and hormonal therapy. Salvage radiotherapy alone was associated with a significant 3-fold increase in prostate cancer-specific survival relative to those who received no salvage treatment (hazard ratio [HR], 0.32 [95% confidence interval {CI}, 0.19-0.54]; P<.001). Addition of hormonal therapy to salvage radiotherapy was not associated with any additional increase in prostate cancer-specific survival (HR, 0.34 [95% CI, 0.17-0.69]; P = .003). The increase in prostate cancer-specific survival associated with salvage radiotherapy was limited to men with a prostate-specific antigen doubling time of less than 6 months and remained after adjustment for pathological stage and other established prognostic factors. Salvage radiotherapy initiated more than 2 years after recurrence provided no significant increase in prostate cancer-specific survival. Men whose prostate-specific antigen level never became undetectable after salvage radiotherapy did not experience a significant increase in prostate cancer-specific survival. Salvage radiotherapy also was associated with a significant increase in overall survival.
Conclusions: Salvage radiotherapy administered within 2 years of biochemical recurrence was associated with a significant increase in prostate cancer-specific survival among men with a prostate-specific antigen doubling time of less than 6 months, independent of other prognostic features such as pathological stage or Gleason score. These preliminary findings should be validated in other settings, and ultimately, in a randomized controlled trial.
Figures
Comment in
-
Adjuvant radiotherapy after surgery for prostate cancer.JAMA. 2008 Nov 12;300(18):2119; author reply 2119. doi: 10.1001/jama.2008.562. JAMA. 2008. PMID: 19001623 No abstract available.
-
Words of wisdom. Re: Prostate cancer-specific survival following salvage radiotherapy versus observation in men with biochemical recurrence after radical prostatectomy. Trock BJ, Han M, Freedland SJ, Humphreys EB, DeWeese TL, Partin AW, Walsh PC. JAMA 2008;299:2760-9.Eur Urol. 2009 Jan;55(1):247. doi: 10.1016/j.eururo.2008.09.034. Eur Urol. 2009. PMID: 20050016 No abstract available.
References
-
- Penson DF, Chan JM. Prostate cancer. J Urol. 2007;177(6):2020–2029. - PubMed
-
- Han M, Partin AW, Pound CR, Epstein JI, Walsh PC. Long-term biochemical disease-free and cancer-specific survival following anatomic radical retropubic prostatectomy: the 15-year Johns Hopkins experience. Urol Clin North Am. 2001;28(3):555–565. - PubMed
-
- Ward JF, Moul JW. Rising prostate-specific antigen after primary prostate cancer therapy. Nat Clin Pract Urol. 2005;2(4):174–182. - PubMed
-
- Pound CR, Partin AW, Eisenberger MA, et al. Natural history of progression after PSA elevation following radical prostatectomy. JAMA. 1999;281(17):1591–1597. - PubMed
-
- Bolla M, van Poppel H, Collette L, et al. European Organization for Research and Treatment of Cancer. Postoperative radiotherapy after radical prostatectomy: a randomised controlled trial (EORTC trial 22911) Lancet. 2005;366(9485):572–578. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
