

Cellular islet autoimmunity associates with clinical outcome of islet cell transplantation
- PMID: 18560516
- PMCID: PMC2426735
- DOI: 10.1371/journal.pone.0002435
Cellular islet autoimmunity associates with clinical outcome of islet cell transplantation
Abstract
Background: Islet cell transplantation can cure type 1 diabetes (T1D), but only a minority of recipients remains insulin-independent in the following years. We tested the hypothesis that allograft rejection and recurrent autoimmunity contribute to this progressive loss of islet allograft function.
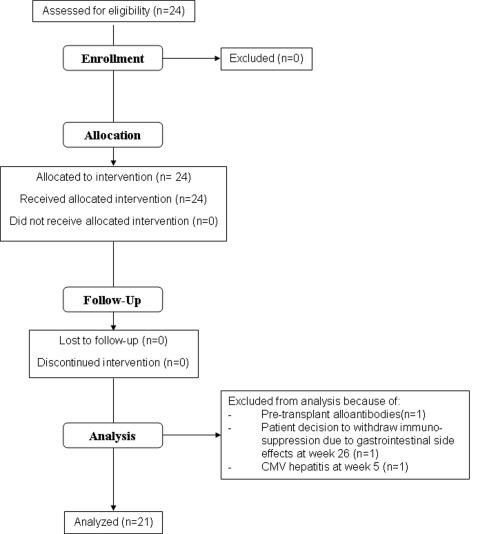
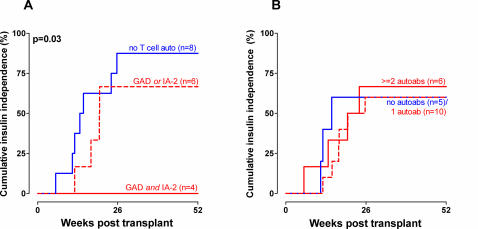
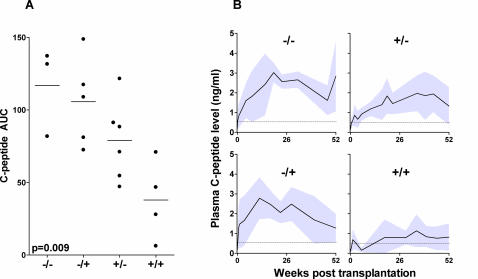
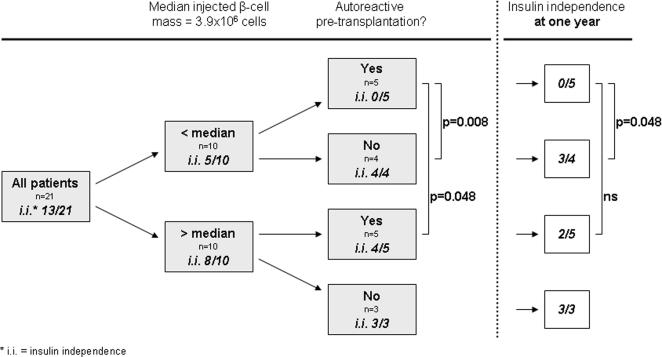
Methodology/principal findings: Twenty-one T1D patients received cultured islet cell grafts prepared from multiple donors and transplanted under anti-thymocyte globulin (ATG) induction and tacrolimus plus mycophenolate mofetil (MMF) maintenance immunosuppression. Immunity against auto- and alloantigens was measured before and during one year after transplantation. Cellular auto- and alloreactivity was assessed by lymphocyte stimulation tests against autoantigens and cytotoxic T lymphocyte precursor assays, respectively. Humoral reactivity was measured by auto- and alloantibodies. Clinical outcome parameters--including time until insulin independence, insulin independence at one year, and C-peptide levels over one year--remained blinded until their correlation with immunological parameters. All patients showed significant improvement of metabolic control and 13 out of 21 became insulin-independent. Multivariate analyses showed that presence of cellular autoimmunity before and after transplantation is associated with delayed insulin-independence (p = 0.001 and p = 0.01, respectively) and lower circulating C-peptide levels during the first year after transplantation (p = 0.002 and p = 0.02, respectively). Seven out of eight patients without pre-existent T-cell autoreactivity became insulin-independent, versus none of the four patients reactive to both islet autoantigens GAD and IA-2 before transplantation. Autoantibody levels and cellular alloreactivity had no significant association with outcome.
Conclusions/significance: In this cohort study, cellular islet-specific autoimmunity associates with clinical outcome of islet cell transplantation under ATG-tacrolimus-MMF immunosuppression. Tailored immunotherapy targeting cellular islet autoreactivity may be required. Monitoring cellular immune reactivity can be useful to identify factors influencing graft survival and to assess efficacy of immunosuppression.
Trial registration: Clinicaltrials.gov NCT00623610.
Conflict of interest statement
Figures
References
-
- Shapiro AM, Lakey JR, Ryan EA, Korbutt GS, Toth E, et al. Islet transplantation in seven patients with type 1 diabetes mellitus using a glucocorticoid-free immunosuppressive regimen. N Engl J Med. 2000;343:230–238. - PubMed
-
- Keymeulen B, Ling Z, Gorus FK, Delvaux G, Bouwens L, et al. Implantation of standardized beta-cell grafts in a liver segment of IDDM patients: graft and recipients characteristics in two cases of insulin-independence under maintenance immunosuppression for prior kidney graft. Diabetologia. 1998;41:452–459. - PubMed
-
- Hering BJ, Kandaswamy R, Harmon JV, Ansite JD, Clemmings SM, et al. Transplantation of cultured islets from two-layer preserved pancreases in type 1 diabetes with anti-CD3 antibody. Am J Transplant. 2004;4:390–401. - PubMed
-
- Ricordi C, Inverardi L, Kenyon NS, Goss J, Bertuzzi F, Alejandro R. Requirements for success in clinical islet transplantation. Transplantation. 2005;79:1298–1300. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
