

Molecular determinants of magnesium homeostasis: insights from human disease
- PMID: 18562569
- PMCID: PMC4959876
- DOI: 10.1681/ASN.2008010098
Molecular determinants of magnesium homeostasis: insights from human disease
Abstract
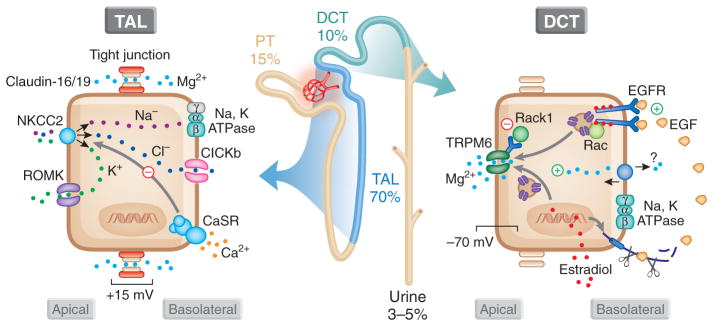
The past decade has witnessed multiple advances in our understanding of magnesium (Mg(2+)) homeostasis. The discovery that mutations in claudin-16/paracellin-1 or claudin-19 are responsible for familial hypomagnesemia with hypercalciuria and nephrocalcinosis provided insight into the molecular mechanisms governing paracellular transport of Mg(2+). Our understanding of the transcellular movement of Mg(2+) was similarly enhanced by the realization that defects in transient receptor potential melastatin 6 (TRPM6) cause hypomagnesemia with secondary hypocalcemia. This channel regulates the apical entry of Mg(2+) into epithelia. In so doing, TRPM6 alters whole-body Mg(2+) homeostasis by controlling urinary excretion. Consequently, investigation into the regulation of TRPM6 has increased. Acid-base status, 17beta estradiol, and the immunosuppressive agents FK506 and cyclosporine affect plasma Mg(2+) levels by altering TRPM6 expression. A mutation in epithelial growth factor is responsible for isolated autosomal recessive hypomagnesemia, and epithelial growth factor activates TRPM6. A defect in the gamma-subunit of the Na,K-ATPase causes isolated dominant hypomagnesemia by altering TRPM6 activity through a decrease in the driving force for apical Mg(2+) influx. We anticipate that the next decade will provide further detail into the control of the gatekeeper TRPM6 and, therefore, overall whole-body Mg(2+) balance.
Figures
References
-
- Elin RJ. Magnesium: The fifth but forgotten electrolyte. Am J Clin Pathol. 1994;102:616–622. - PubMed
-
- Flatman PW. Magnesium transport across cell membranes. J Membr Biol. 1984;80:1–14. - PubMed
-
- Quamme GA. Renal handling of magnesium: Drug and hormone interactions. Magnesium. 1986;5:248–272. - PubMed
-
- Topf JM, Murray PT. Hypomagnesemia and hypermagnesemia. Rev Endocr Metab Disord. 2003;4:195–206. - PubMed
-
- Tong GM, Rude RK. Magnesium deficiency in critical illness. J Intensive Care Med. 2005;20:3–17. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
