

Lifetime cost-effectiveness of calcineurin inhibitor withdrawal after de novo renal transplantation
- PMID: 18562571
- PMCID: PMC2518430
- DOI: 10.1681/ASN.2007040495
Lifetime cost-effectiveness of calcineurin inhibitor withdrawal after de novo renal transplantation
Abstract
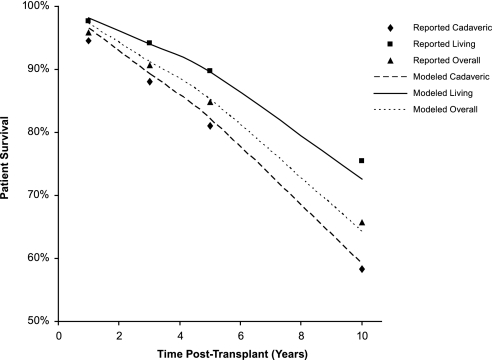
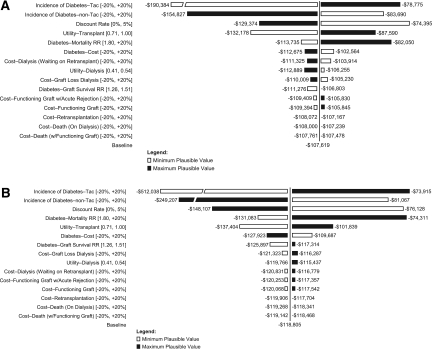
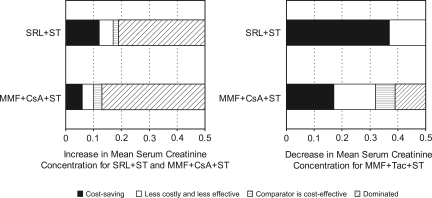
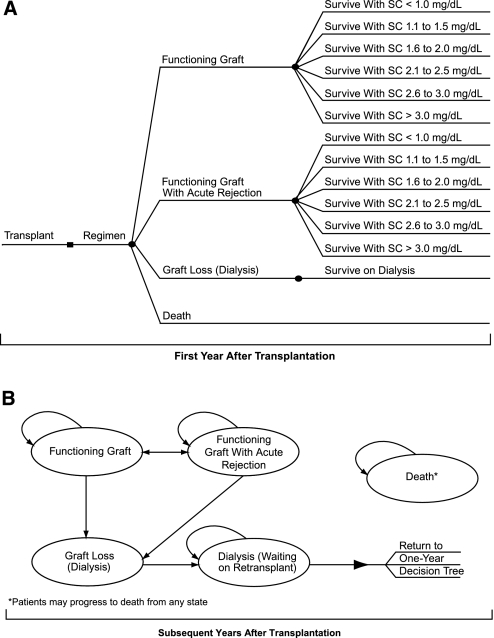
After renal transplantation, immunosuppressive regimens associated with high short-term survival rates are not necessarily associated with high long-term survival rates, suggesting that regimens may need to be optimized over time. Calcineurin inhibitor (CNI) withdrawal from a sirolimus-based immunosuppressive regimen may maximize the likelihood of long-term graft and patient survival by minimizing CNI-associated nephrotoxicity. In this study, a lifetime Markov model was created to compare the cost-effectiveness of a sirolimus-based CNI withdrawal regimen (sirolimus plus steroids) with other common CNI-containing regimens in adult de novo renal transplantation patients. Long-term graft survival was estimated by renal function and data from published studies and the US transplant registry, including short- and long-term outcomes, utility weights, and health-state costs were incorporated. Drug costs were based on average daily consumption and wholesale acquisition costs. The model suggests that treatment with sirolimus plus steroids is more efficacious and less costly than regimens consisting of a CNI, mycophenolate mofetil, and steroids; therefore, CNI withdrawal not only shows potential for long-term clinical benefits but also is expected to be cost-saving over a patient's life compared with the most commonly prescribed CNI-containing regimens.
Figures
Comment in
-
The practical utility of an economic analysis of calcineurin withdrawal following renal transplantation.J Am Soc Nephrol. 2008 Sep;19(9):1627-8. doi: 10.1681/ASN.2008070723. Epub 2008 Aug 6. J Am Soc Nephrol. 2008. PMID: 18684891 No abstract available.
Similar articles
-
Calcineurin inhibitor-sparing regimens in solid organ transplantation: focus on improving renal function and nephrotoxicity.Clin Transplant. 2008 Jan-Feb;22(1):1-15. doi: 10.1111/j.1399-0012.2007.00739.x. Clin Transplant. 2008. PMID: 18217899 Review.
-
A Randomized 2x2 Factorial Clinical Trial of Renal Transplantation: Steroid-Free Maintenance Immunosuppression with Calcineurin Inhibitor Withdrawal after Six Months Associates with Improved Renal Function and Reduced Chronic Histopathology.PLoS One. 2015 Oct 14;10(10):e0139247. doi: 10.1371/journal.pone.0139247. eCollection 2015. PLoS One. 2015. PMID: 26465152 Free PMC article. Clinical Trial.
-
Calcineurin inhibitor sparing in paediatric solid organ transplantation : managing the efficacy/toxicity conundrum.Drugs. 2008;68(10):1385-414. doi: 10.2165/00003495-200868100-00004. Drugs. 2008. PMID: 18578558 Review.
-
Treatment strategies in pediatric solid organ transplant recipients with calcineurin inhibitor-induced nephrotoxicity.Pediatr Transplant. 2006 Sep;10(6):721-9. doi: 10.1111/j.1399-3046.2006.00577.x. Pediatr Transplant. 2006. PMID: 16911497 Review.
-
High incidence of rejection episodes and poor tolerance of sirolimus in a protocol with early steroid withdrawal and calcineurin inhibitor-free maintenance therapy in renal transplantation: experiences of a randomized prospective single-center study.Transplant Proc. 2012 Dec;44(10):2961-5. doi: 10.1016/j.transproceed.2012.07.142. Transplant Proc. 2012. PMID: 23195006 Clinical Trial.
Cited by
-
A prospective, multinational pharmacoepidemiological study of clinical conversion to sirolimus immunosuppression after renal transplantation.J Transplant. 2012;2012:107180. doi: 10.1155/2012/107180. Epub 2012 Aug 9. J Transplant. 2012. PMID: 22934151 Free PMC article.
-
Estimating Health-State Utility Values in Kidney Transplant Recipients and Waiting-List Patients Using the EQ-5D-5L.Value Health. 2017 Jul-Aug;20(7):976-984. doi: 10.1016/j.jval.2017.01.011. Epub 2017 May 12. Value Health. 2017. PMID: 28712628 Free PMC article.
-
Cost-effectiveness of modern mTOR inhibitor based immunosuppression compared to the standard of care after renal transplantation in Germany.Eur J Health Econ. 2015 May;16(4):377-90. doi: 10.1007/s10198-014-0579-3. Epub 2014 Apr 13. Eur J Health Econ. 2015. PMID: 24728542
-
The Cost of Transplant Immunosuppressant Therapy: Is This Sustainable?Curr Transplant Rep. 2015 Jun 1;2(2):113-121. doi: 10.1007/s40472-015-0052-y. Curr Transplant Rep. 2015. PMID: 26236578 Free PMC article.
-
Immune monitoring as prerequisite for transplantation tolerance trials.Clin Exp Immunol. 2017 Aug;189(2):158-170. doi: 10.1111/cei.12988. Epub 2017 Jun 23. Clin Exp Immunol. 2017. PMID: 28518214 Free PMC article. Review.
References
-
- Kasiske BL, Vazquez MA, Harmon WE, Brown RS, Danovitch GM, Gaston RS, Roth D, Scandling SD Jr, Singer GG: Recommendations for the outpatient surveillance of renal transplant recipients. J Am Soc Nephrol 11[Suppl 15]: S1–S86, 2000 - PubMed
-
- Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, Held PJ, Port FK: Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med 341: 1725–1730, 1999 - PubMed
-
- Mulay AV, Hussain N, Fergusson D, Knoll BA: Calcineurin inhibitor withdrawal from sirolimus-based therapy in kidney transplantation: A systematic review of randomized trials. Am J Transplant 5: 1748–1756, 2005 - PubMed
-
- Kreis H, Oberbauer R, Campistol JM, Mather T, Daloze P, Schena FP, Burke JT, Brault Y, Gioud-Paquet M, Scarola JA, Neylan JF: Long-term benefits with sirolimus-based therapy after early cyclosporine withdrawal. J Am Soc Nephrol 15: 809–817, 2004 - PubMed
-
- Oberbauer R, Kreis H, Johnson RW, Mota A, Claesson K, Ruiz JC, Wilczek H, Jamieson N, Henriques AC, Paczek L, Chapman J, Burke JT: Long-term improvement in renal function with sirolimus after early cyclosporine withdrawal in renal transplant recipients: 2-Year results of the Rapamune maintenance regimen study. Transplantation 76: 364–370, 2003 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
