

Endorectal ultrasonography versus phased-array magnetic resonance imaging for preoperative staging of rectal cancer
- PMID: 18567078
- PMCID: PMC2716612
- DOI: 10.3748/wjg.14.3504
Endorectal ultrasonography versus phased-array magnetic resonance imaging for preoperative staging of rectal cancer
Abstract
Aim: To compare the diagnostic accuracy of pelvic phased-array magnetic resonance imaging (MRI) and endorectal ultrasonography (ERUS) in the preoperative staging of rectal carcinoma.
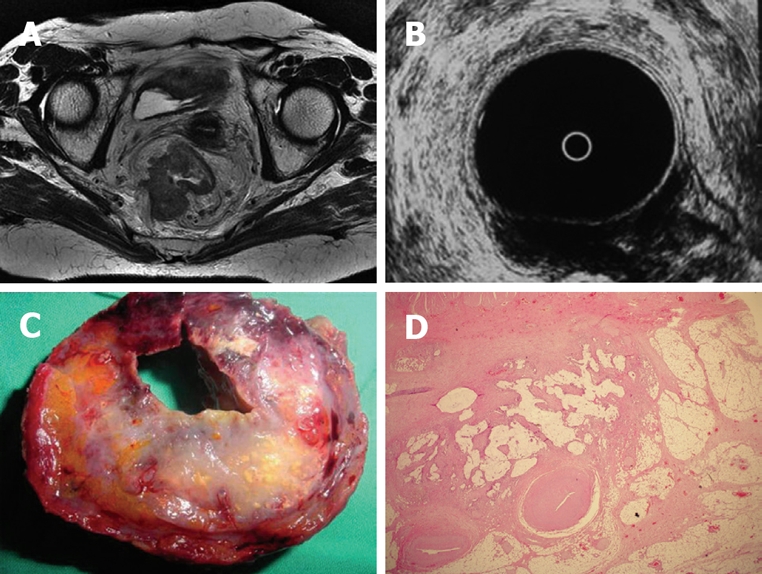
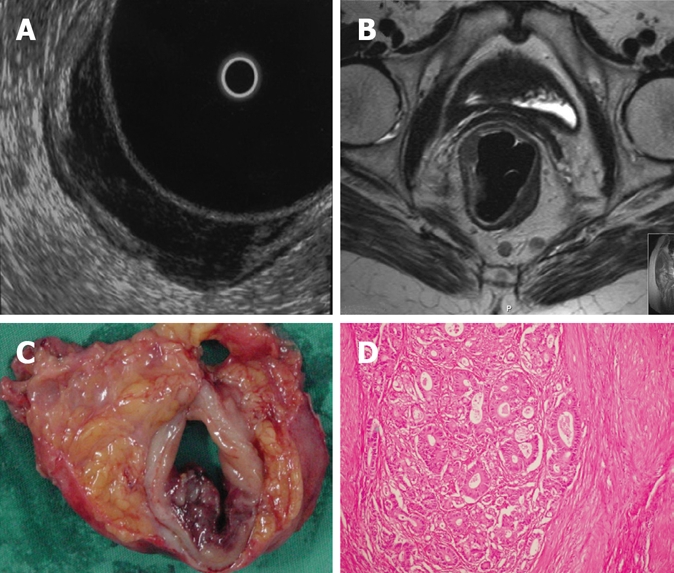
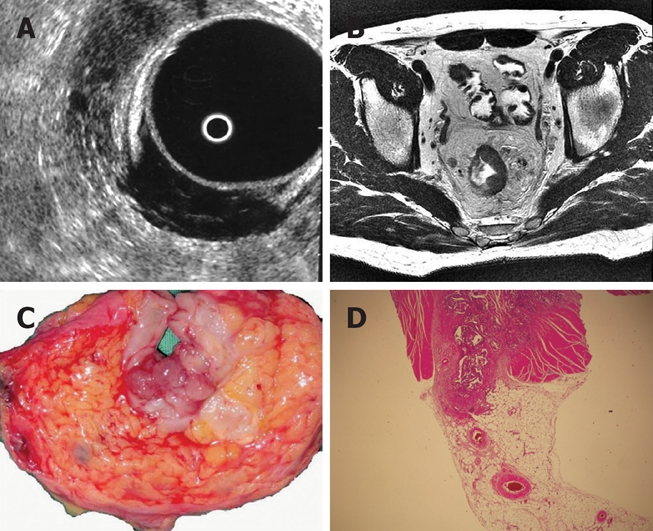
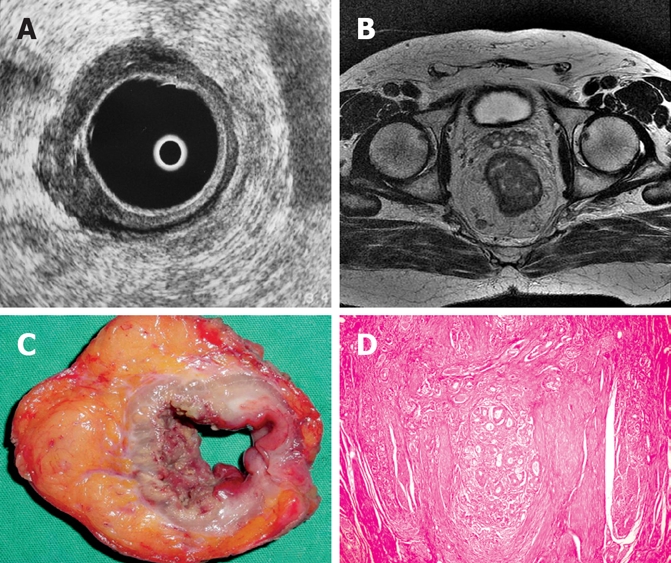
Methods: Thirty-four patients (15 males, 19 females) with ages ranging between 29 and 75 who have biopsy proven rectal tumor underwent both MRI and ERUS examinations before surgery. All patients were evaluated to determine the diagnostic accuracy of depth of transmural tumor invasion and lymph node metastases. Imaging results were correlated with histopathological findings regarded as the gold standard and both modalities were compared in terms of predicting preoperative local staging of rectal carcinoma.
Results: The pathological T stage of the tumors was: pT1 in 1 patient, pT2 in 9 patients, pT3 in 21 patients and pT4 in 3 patients. The pathological N stage of the tumors was: pN0 in 19 patients, pN1 in 9 patients and pN2 in 6 patients. The accuracy of T staging for MRI was 89.70% (27 out of 34). The sensitivity was 79.41% and the specificity was 93.14%. The accuracy of T staging for ERUS was 85.29% (24 out of 34). The sensitivity was 70.59% and the specificity was 90.20%. Detection of lymph node metastases using phased-array MRI gave an accuracy of 74.50% (21 out of 34). The sensitivity and specificity was found to be 61.76% and 80.88%, respectively. By using ERUS in the detection of lymph node metastases, an accuracy of 76.47% (18 out of 34) was obtained. The sensitivity and specificity were found to be 52.94% and 84.31%, respectively.
Conclusion: ERUS and phased-array MRI are complementary methods in the accurate preoperative staging of rectal cancer. In conclusion, we can state that phased-array MRI was observed to be slightly superior in determining the depth of transmural invasion (T stage) and has same value in detecting lymph node metastases (N stage) as compared to ERUS.
Figures
Similar articles
-
[Comparative study of endorectal ultrasonography and magnetic resonance imaging in preoperative staging of rectal cancer].Zhonghua Yi Xue Za Zhi. 2014 May 6;94(17):1318-21. Zhonghua Yi Xue Za Zhi. 2014. PMID: 25142852 Chinese.
-
[Clinical value of radial endorectal ultrasound in the assessment of preoperative staging of rectal carcinoma].Zhonghua Zhong Liu Za Zhi. 2013 Feb;35(2):148-53. doi: 10.3760/cma.j.issn.0253-3766.2013.02.017. Zhonghua Zhong Liu Za Zhi. 2013. PMID: 23714673 Chinese.
-
Accuracy of thin-section magnetic resonance imaging with a pelvic phased-array coil in the local staging of rectal cancer.J Comput Assist Tomogr. 2013 Jan-Feb;37(1):58-64. doi: 10.1097/RCT.0b013e3182772ec5. J Comput Assist Tomogr. 2013. PMID: 23321834
-
Endorectal ultrasound in the preoperative evaluation of rectal cancer.Clin Colorectal Cancer. 2004 Jul;4(2):124-32. doi: 10.3816/ccc.2004.n.015. Clin Colorectal Cancer. 2004. PMID: 15285819 Review.
-
The accuracy of MRI, endorectal ultrasonography, and computed tomography in predicting the response of locally advanced rectal cancer after preoperative therapy: A metaanalysis.Surgery. 2016 Mar;159(3):688-99. doi: 10.1016/j.surg.2015.10.019. Epub 2015 Nov 24. Surgery. 2016. PMID: 26619929 Review.
Cited by
-
Staging anal cancer: prospective comparison of transanal endoscopic ultrasound and magnetic resonance imaging.J Gastrointest Surg. 2009 Jul;13(7):1292-8. doi: 10.1007/s11605-009-0870-2. Epub 2009 Apr 14. J Gastrointest Surg. 2009. PMID: 19365694
-
Gastrointestinal imaging-practical magnetic resonance imaging approach.World J Radiol. 2014 Aug 28;6(8):544-66. doi: 10.4329/wjr.v6.i8.544. World J Radiol. 2014. PMID: 25170393 Free PMC article. Review.
-
Squamous cell carcinoma arising from long-standing perianal fistula.Int Wound J. 2010 Dec;7(6):515-8. doi: 10.1111/j.1742-481X.2010.00724.x. Epub 2010 Aug 19. Int Wound J. 2010. PMID: 20726921 Free PMC article.
-
Magnetic Resonance Imaging Evaluation of the Accuracy of Various Lymph Node Staging Criteria in Rectal Cancer: A Systematic Review and Meta-Analysis.Front Oncol. 2021 Jul 13;11:709070. doi: 10.3389/fonc.2021.709070. eCollection 2021. Front Oncol. 2021. PMID: 34327144 Free PMC article.
-
A computer-aided algorithm to quantitatively predict lymph node status on MRI in rectal cancer.Br J Radiol. 2012 Sep;85(1017):1272-8. doi: 10.1259/bjr/13374146. Br J Radiol. 2012. PMID: 22919008 Free PMC article.
References
-
- Lindmark G, Gerdin B, Pahlman L, Bergstrom R, Glimelius B. Prognostic predictors in colorectal cancer. Dis Colon Rectum. 1994;37:1219–1227. - PubMed
-
- Moriya Y, Sugihara K, Akasu T, Fujita S. Patterns of recurrence after nerve-sparing surgery for rectal adenocarcinoma with special reference to loco-regional recurrence. Dis Colon Rectum. 1995;38:1162–1168. - PubMed
-
- Heriot AG, Hicks RJ, Drummond EG, Keck J, Mackay J, Chen F, Kalff V. Does positron emission tomography change management in primary rectal cancer? A prospective assessment. Dis Colon Rectum. 2004;47:451–458. - PubMed
-
- Dobos N, Rubesin SE. Radiologic imaging modalities in the diagnosis and management of colorectal cancer. Hematol Oncol Clin North Am. 2002;16:875–895. - PubMed
-
- Ahmad NA, Kochman ML, Ginsberg GG. Endoscopic ultrasound and endoscopic mucosal resection for rectal cancers and villous adenomas. Hematol Oncol Clin North Am. 2002;16:897–906. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
