

Review
doi: 10.1151/spp021113.
The neurobiology of opioid dependence: implications for treatment
Affiliations
- PMID: 18567959
- PMCID: PMC2851054
- DOI: 10.1151/spp021113
Item in Clipboard
Review
The neurobiology of opioid dependence: implications for treatment
Sci Pract Perspect.
2002 Jul.
Abstract
Opioid tolerance, dependence, and addiction are all manifestations of brain changes resulting from chronic opioid abuse. The opioid abuser's struggle for recovery is in great part a struggle to overcome the effects of these changes. Medications such as methadone, LAAM, buprenorphine, and naltrexone act on the same brain structures and processes as addictive opioids, but with protective or normalizing effects. Despite the effectiveness of medications, they must be used in conjunction with appropriate psychosocial treatments.
Figures
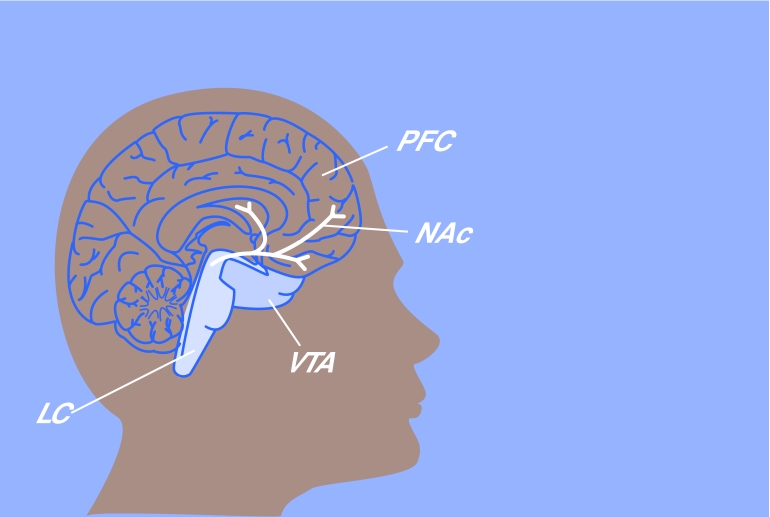
When drugs stimulate mu opioid receptors in the brain, cells in the ventral tegmental area (VTA) produce dopamine and release it into the nucleus accumbens (NAc), giving rise to feelings of pleasure. Feedback from the prefrontal cortex (PFC) to the VTA helps us overcome drives to obtain pleasure through actions that may be unsafe or unwise, but this feedback appears to be compromised in individuals who become addicted to drugs. The locus ceruleus (LC) is an area of the brain that plays an important role in drug dependence.
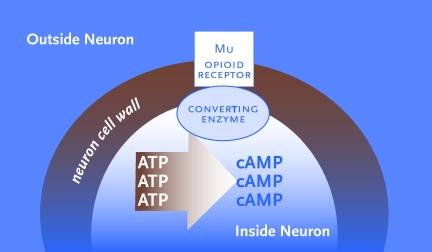
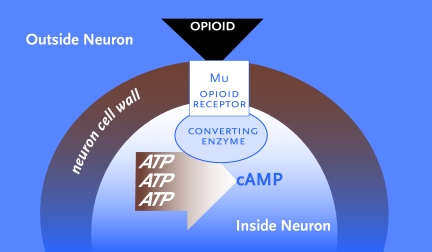
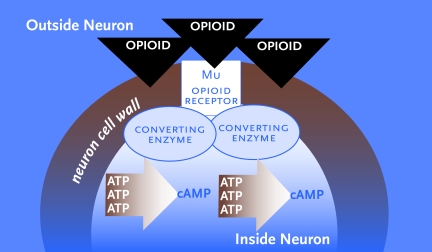
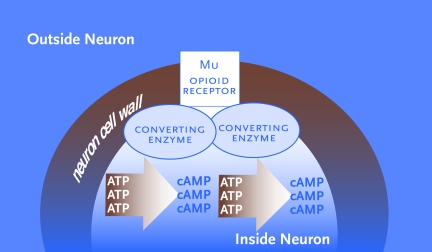
The locus ceruleus (LC) is an area of the brain that is critically involved in the production of opioid dependence and withdrawal. The diagrams show how opioid drugs affect processes in the LC that control the release of noradrenaline (NA), a brain chemical that stimulates wakefulness, muscle tone, and respiration, among other functions. A. Normally, natural opiatelike chemicals produced by the body link to mu opioid receptors on the surface of neurons. This linkage activates an enzyme that converts a chemical called adenosine triphosphate (ATP) into another chemical, called cyclic adenosine monophosphate (cAMP), which in turn triggers the release of NA. Prior to initiation of opioid drug abuse, the neuron produces enough NA to maintain normal levels of alertness, muscle tone, respiration, etc. B. When heroin or another opioid drug links to the mu opioid receptors, it inhibits the enzyme that converts ATP to cAMP. As a result, less cAMP is produced, less NA is released. Alertness, muscle tone, and respiration drop, and the acute opioid effects of sedation, shallow breathing, etc., appear. C. With repeated heroin exposure, the neuron increases its supply of enzyme and ATP molecules. Using these extra raw materials, the neuron can produce enough cAMP to offset the inhibitory effect of the drug and release roughly normal amounts of NA despite the presence of the drug. At this stage, the individual no longer experiences the same intensity of acute opioid effects as in earlier stages of abuse. D. When heroin is discontinued after chronic abuse, the drug’s inhibitory impact is lost. Operating at normal efficiency but with enhanced supplies of converting enzyme and ATP, the neuron produces abnormally high levels of cAMP, leading to excessive release of NA. The patient experiences the clinical symptoms of withdrawal—jitters, anxiety, muscle cramps, etc. If no further drugs are taken, the neuron will largely revert to its predrug condition (panel A) within days or weeks.
The locus ceruleus (LC) is an area of the brain that is critically involved in the production of opioid dependence and withdrawal. The diagrams show how opioid drugs affect processes in the LC that control the release of noradrenaline (NA), a brain chemical that stimulates wakefulness, muscle tone, and respiration, among other functions. A. Normally, natural opiatelike chemicals produced by the body link to mu opioid receptors on the surface of neurons. This linkage activates an enzyme that converts a chemical called adenosine triphosphate (ATP) into another chemical, called cyclic adenosine monophosphate (cAMP), which in turn triggers the release of NA. Prior to initiation of opioid drug abuse, the neuron produces enough NA to maintain normal levels of alertness, muscle tone, respiration, etc. B. When heroin or another opioid drug links to the mu opioid receptors, it inhibits the enzyme that converts ATP to cAMP. As a result, less cAMP is produced, less NA is released. Alertness, muscle tone, and respiration drop, and the acute opioid effects of sedation, shallow breathing, etc., appear. C. With repeated heroin exposure, the neuron increases its supply of enzyme and ATP molecules. Using these extra raw materials, the neuron can produce enough cAMP to offset the inhibitory effect of the drug and release roughly normal amounts of NA despite the presence of the drug. At this stage, the individual no longer experiences the same intensity of acute opioid effects as in earlier stages of abuse. D. When heroin is discontinued after chronic abuse, the drug’s inhibitory impact is lost. Operating at normal efficiency but with enhanced supplies of converting enzyme and ATP, the neuron produces abnormally high levels of cAMP, leading to excessive release of NA. The patient experiences the clinical symptoms of withdrawal—jitters, anxiety, muscle cramps, etc. If no further drugs are taken, the neuron will largely revert to its predrug condition (panel A) within days or weeks.
The locus ceruleus (LC) is an area of the brain that is critically involved in the production of opioid dependence and withdrawal. The diagrams show how opioid drugs affect processes in the LC that control the release of noradrenaline (NA), a brain chemical that stimulates wakefulness, muscle tone, and respiration, among other functions. A. Normally, natural opiatelike chemicals produced by the body link to mu opioid receptors on the surface of neurons. This linkage activates an enzyme that converts a chemical called adenosine triphosphate (ATP) into another chemical, called cyclic adenosine monophosphate (cAMP), which in turn triggers the release of NA. Prior to initiation of opioid drug abuse, the neuron produces enough NA to maintain normal levels of alertness, muscle tone, respiration, etc. B. When heroin or another opioid drug links to the mu opioid receptors, it inhibits the enzyme that converts ATP to cAMP. As a result, less cAMP is produced, less NA is released. Alertness, muscle tone, and respiration drop, and the acute opioid effects of sedation, shallow breathing, etc., appear. C. With repeated heroin exposure, the neuron increases its supply of enzyme and ATP molecules. Using these extra raw materials, the neuron can produce enough cAMP to offset the inhibitory effect of the drug and release roughly normal amounts of NA despite the presence of the drug. At this stage, the individual no longer experiences the same intensity of acute opioid effects as in earlier stages of abuse. D. When heroin is discontinued after chronic abuse, the drug’s inhibitory impact is lost. Operating at normal efficiency but with enhanced supplies of converting enzyme and ATP, the neuron produces abnormally high levels of cAMP, leading to excessive release of NA. The patient experiences the clinical symptoms of withdrawal—jitters, anxiety, muscle cramps, etc. If no further drugs are taken, the neuron will largely revert to its predrug condition (panel A) within days or weeks.
The locus ceruleus (LC) is an area of the brain that is critically involved in the production of opioid dependence and withdrawal. The diagrams show how opioid drugs affect processes in the LC that control the release of noradrenaline (NA), a brain chemical that stimulates wakefulness, muscle tone, and respiration, among other functions. A. Normally, natural opiatelike chemicals produced by the body link to mu opioid receptors on the surface of neurons. This linkage activates an enzyme that converts a chemical called adenosine triphosphate (ATP) into another chemical, called cyclic adenosine monophosphate (cAMP), which in turn triggers the release of NA. Prior to initiation of opioid drug abuse, the neuron produces enough NA to maintain normal levels of alertness, muscle tone, respiration, etc. B. When heroin or another opioid drug links to the mu opioid receptors, it inhibits the enzyme that converts ATP to cAMP. As a result, less cAMP is produced, less NA is released. Alertness, muscle tone, and respiration drop, and the acute opioid effects of sedation, shallow breathing, etc., appear. C. With repeated heroin exposure, the neuron increases its supply of enzyme and ATP molecules. Using these extra raw materials, the neuron can produce enough cAMP to offset the inhibitory effect of the drug and release roughly normal amounts of NA despite the presence of the drug. At this stage, the individual no longer experiences the same intensity of acute opioid effects as in earlier stages of abuse. D. When heroin is discontinued after chronic abuse, the drug’s inhibitory impact is lost. Operating at normal efficiency but with enhanced supplies of converting enzyme and ATP, the neuron produces abnormally high levels of cAMP, leading to excessive release of NA. The patient experiences the clinical symptoms of withdrawal—jitters, anxiety, muscle cramps, etc. If no further drugs are taken, the neuron will largely revert to its predrug condition (panel A) within days or weeks.
Comment in
-
Response: the neurobiological model in community treatment programs.Sci Pract Perspect. 2002 Jul;1(1):21. doi: 10.1151/spp021121. Sci Pract Perspect. 2002. PMID: 18567960 Free PMC article. No abstract available.
References
-
- Behar KL, et al. Preliminary evidence of low cortical GABA levels in localized 1H-MR spectra of alcohol-dependent and hepatic encephalopathy patients. American Journal of Psychiatry. 1999;156(6):952–954. - PubMed
-
- Breiter HC, et al. Acute effects of cocaine on human brain activity and emotion. Neuron. 1997;19(3):591–611. - PubMed
-
- Dole VP, Nyswander ME, Kreek MJ. Narcotic blockade. Archives of Internal Medicine. 1966;118(4):304–309. - PubMed
-
- Grace AA. The tonic/phasic model of dopamine system regulation and its implications for understanding alcohol and stimulant craving. Addiction. 2000;95(Suppl 2):S119–S128. - PubMed
-
- Judd LL, et al. Effective medical treatment of opiate addiction. Journal of the American Medical Association. 1998;280(22):1936–1943.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical