

What role may symptoms play in the diagnosis of airflow limitation? A study in an elderly population
- PMID: 18570007
- PMCID: PMC3406655
- DOI: 10.1080/02813430802028938
What role may symptoms play in the diagnosis of airflow limitation? A study in an elderly population
Abstract
Background: Chronic obstructive pulmonary disease (COPD) is an under-diagnosed condition. General practitioners meet and examine the patients in early stages of the disease, and symptoms represent the starting point of the diagnostic process.
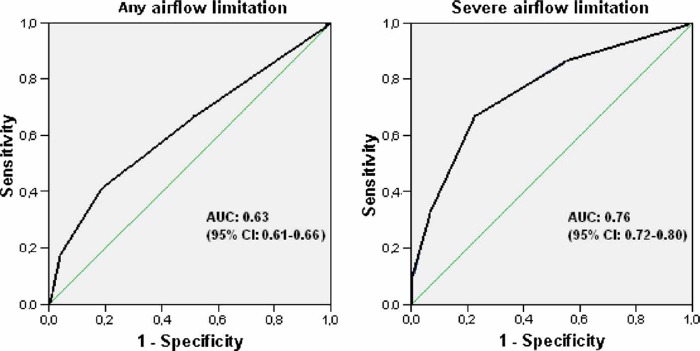
Aim: To evaluate the diagnostic value of respiratory symptoms in the diagnosis of airflow limitation.
Methods: Spirometry was performed in a cross-sectional population-based study of 3954 subjects 60 years and older (54.5% women), who also filled in a questionnaire on symptoms.
Results: The prevalence of any airflow limitation was 15.5% and 20.8%, in women and men, respectively, whereas the corresponding prevalence of severe airflow limitation (FEV(1)<50% predicted) was 3.4% and 4.9%. The positive predictive value of chronic cough with phlegm for any airflow limitation was 37.0% in women and 40.4% in men, and 17.3% and 14.2%, respectively, for severe airflow limitation. Wheezing was a symptom which persisted despite smoking cessation, whereas coughing was considerably less common in ex-smokers than in current smokers. Wheezing, dyspnoea on unhurried walking, dyspnoea on quick walking, and coughing with phlegm were independent predictors of any airflow limitation, OR 1.5, 1.8, 1.4, and 1.6 respectively. (The ORs for severe airflow limitation were 2.4, 2.4, 2.4, and 1.6 respectively.) To be an ex-smoker (OR 2.4) or a current smoker (OR 5.8) was of greater importance. In never- and ex-smokers the chance of having airflow limitation was almost doubled when having two or more, compared with one, of the three symptoms: wheezing, dyspnoea, and coughing with phlegm. Ex-smokers reporting two symptoms had a similar risk of airflow limitation to current smokers not reporting any symptoms.
Conclusion: Respiratory symptoms are valuable predictors of airflow limitation and should be emphasized when selecting patients for spirometry.
Figures
References
-
- Lenfant Claude, Khaltaev Nikolai., editors. Global initiative for Chronic Obstructive Lung Disease, Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease NHLBI/WHO workshop report. 2701; National Institutes of Health, National Heart, Lung, and Blood Institute. 2001; 2005.
-
- Sullivan SD, Buist AS, Weiss K. Health outcomes assessment and economic evaluation in COPD: Challenges and opportunities. Eur Respir J. 2003;21:1S–3S. - PubMed
-
- Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet. 1997;349:1498–1504. - PubMed
-
- Rabe KF, Hurd S, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2007;176:532–55. - PubMed
-
- Pierson DJ. Clinical practice guidelines for chronic obstructive pulmonary disease: A review and comparison of current resources. Respir Care. 2006;51:277–88. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical