

Absence of a proximal to distal gradient of motor deficits in the upper extremity early after stroke
- PMID: 18571981
- PMCID: PMC2584445
- DOI: 10.1016/j.clinph.2008.04.293
Absence of a proximal to distal gradient of motor deficits in the upper extremity early after stroke
Abstract
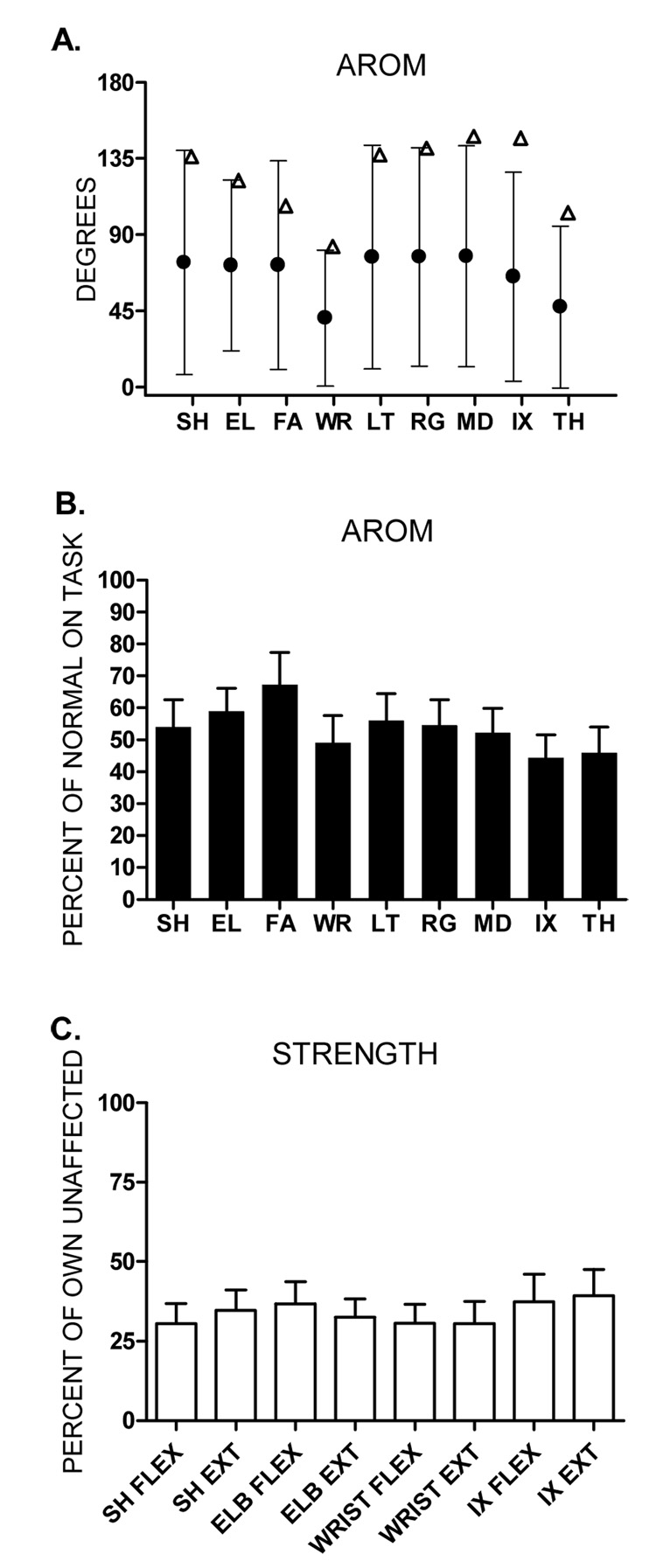
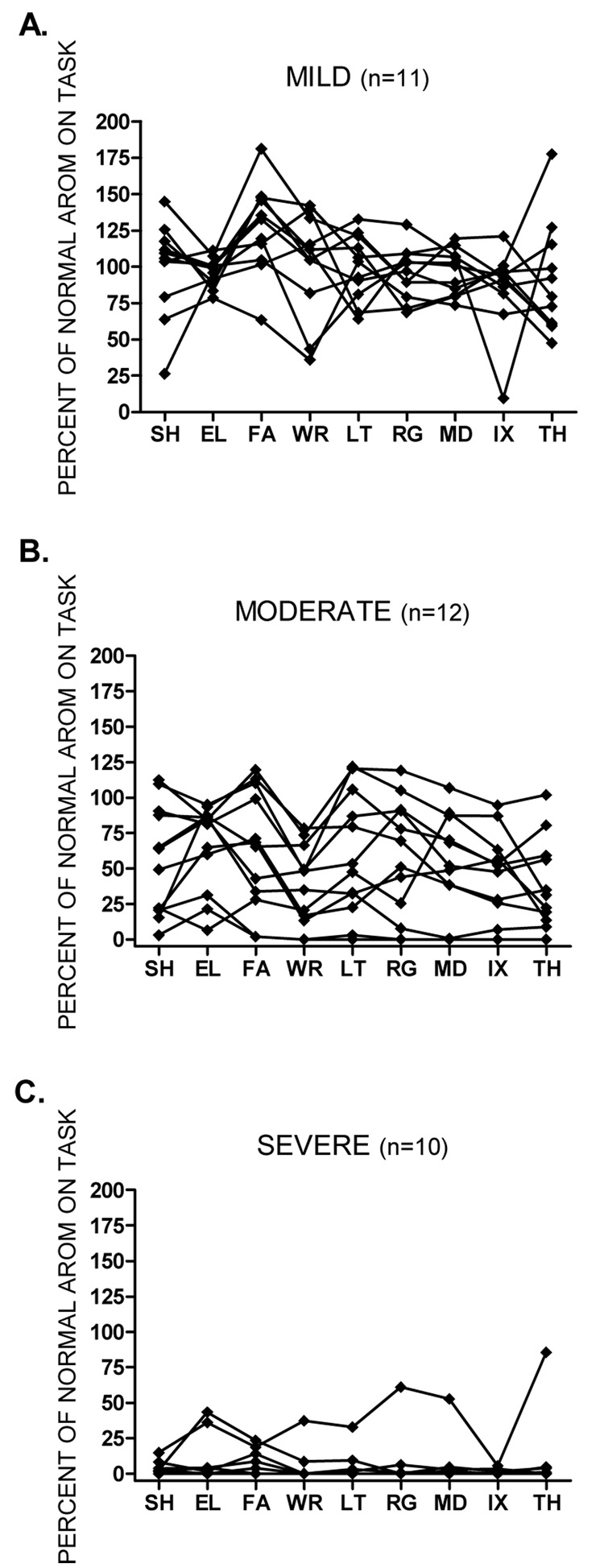
Objective: Our first purpose was to determine whether there was a proximal to distal gradient in motor deficits in nine segments of the affected upper extremity (shoulder, elbow, forearm, wrist, and five fingers) post-stroke. Our second purpose was to determine which upper extremity segments made the greatest contributions to hand function.
Methods: Thirty-three subjects were tested on average 18.6 (+/-5.6) days after stroke. The ability to move each segment was measured by active range of motion (AROM). Hand function was measured by a battery of standardized clinical tests which were synthesized into a single, sensitive score for hand function using principal component analysis.
Results: AROM at all nine segments of the upper extremity was reduced and there was no evidence of a proximal to distal gradient in AROM values. Strength of each segment was reduced and there was also no evidence of a gradient in strength values. AROM at each segment was strongly correlated with hand function scores (range 0.76-0.94). General multiple regression analysis showed that AROM explained 82% of the variance in hand function, with most of the variance shared across proximal, middle, and distal segments. Hierarchical regression analysis showed that shoulder AROM alone could explain 88% of the variance in hand function.
Conclusions: Early after stroke a proximal to distal gradient of motor deficits was not present, and loss of hand function was due to a loss of ability to move many segments of the upper extremity and not just the distal ones.
Significance: These results suggest that a change in the clinical perception of motor deficits post-stroke is needed. Our finding that shoulder AROM predicted almost all the variance in hand function opens up the possibility that this quick, simple measure may be predictive of future hand function. This would be of high economic and clinical utility compared to other ongoing efforts attempting to predict outcomes post-stroke (e.g. fMRI, MEG).
Figures
References
-
- Agnew PJ, Maas F. Hand function related to age and sex. Archives of Physical Medicine and Rehabilitation. 1982;63:269–271. - PubMed
-
- Andrews AW, Thomas MW, Bohannon RW. Normative values for isometric muscle force measurements obtained with hand-held dynamometers. Phys Ther. 1996;76:248–259. - PubMed
-
- Bard G, Hirschberg GG. Recovery of voluntary motionin upper extremity following hemiplegia. Arch Phys Med Rehabil. 1965;46:567–567. - PubMed
-
- Beer RF, Dewald JP, Dawson ML, Rymer WZ. Target-dependent differences between free and constrained arm movements in chronic hemiparesis. Experimental Brain Research. 2004;156:458–470. - PubMed
-
- Beer RF, Dewald JP, Rymer WZ. Deficits in the coordination of multijoint arm movements in patients with hemiparesis: evidence for disturbed control of limb dynamics. Experimental Brain Research. 2000;131:305–319. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
