

Predicting cardiovascular risk in England and Wales: prospective derivation and validation of QRISK2
- PMID: 18573856
- PMCID: PMC2440904
- DOI: 10.1136/bmj.39609.449676.25
Predicting cardiovascular risk in England and Wales: prospective derivation and validation of QRISK2
Abstract
Objective: To develop and validate version two of the QRISK cardiovascular disease risk algorithm (QRISK2) to provide accurate estimates of cardiovascular risk in patients from different ethnic groups in England and Wales and to compare its performance with the modified version of Framingham score recommended by the National Institute for Health and Clinical Excellence (NICE).
Design: Prospective open cohort study with routinely collected data from general practice, 1 January 1993 to 31 March 2008.
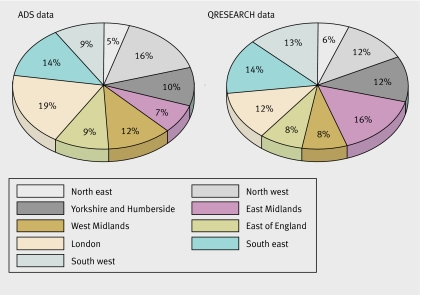
Setting: 531 practices in England and Wales contributing to the national QRESEARCH database.
Participants: 2.3 million patients aged 35-74 (over 16 million person years) with 140,000 cardiovascular events. Overall population (derivation and validation cohorts) comprised 2.22 million people who were white or whose ethnic group was not recorded, 22,013 south Asian, 11,595 black African, 10,402 black Caribbean, and 19,792 from Chinese or other Asian or other ethnic groups.
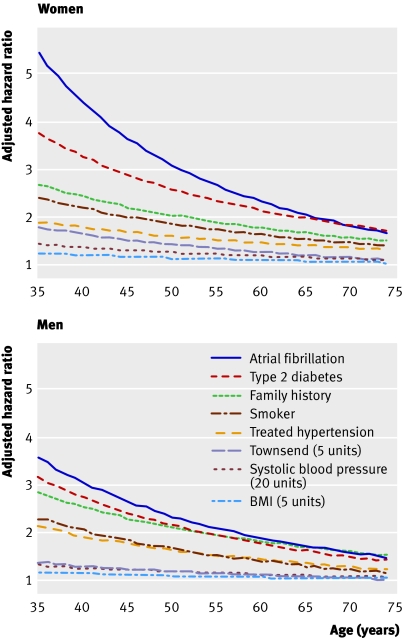
Main outcome measures: First (incident) diagnosis of cardiovascular disease (coronary heart disease, stroke, and transient ischaemic attack) recorded in general practice records or linked Office for National Statistics death certificates. Risk factors included self assigned ethnicity, age, sex, smoking status, systolic blood pressure, ratio of total serum cholesterol:high density lipoprotein cholesterol, body mass index, family history of coronary heart disease in first degree relative under 60 years, Townsend deprivation score, treated hypertension, type 2 diabetes, renal disease, atrial fibrillation, and rheumatoid arthritis.
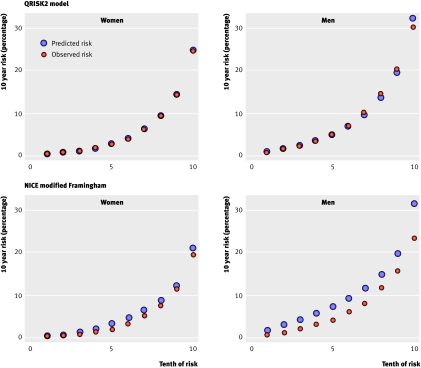
Results: The validation statistics indicated that QRISK2 had improved discrimination and calibration compared with the modified Framingham score. The QRISK2 algorithm explained 43% of the variation in women and 38% in men compared with 39% and 35%, respectively, by the modified Framingham score. Of the 112,156 patients classified as high risk (that is, >or=20% risk over 10 years) by the modified Framingham score, 46,094 (41.1%) would be reclassified at low risk with QRISK2. The 10 year observed risk among these reclassified patients was 16.6% (95% confidence interval 16.1% to 17.0%)-that is, below the 20% treatment threshold. Of the 78 024 patients classified at high risk on QRISK2, 11,962 (15.3%) would be reclassified at low risk by the modified Framingham score. The 10 year observed risk among these patients was 23.3% (22.2% to 24.4%)-that is, above the 20% threshold. In the validation cohort, the annual incidence rate of cardiovascular events among those with a QRISK2 score of >or=20% was 30.6 per 1000 person years (29.8 to 31.5) for women and 32.5 per 1000 person years (31.9 to 33.1) for men. The corresponding figures for the modified Framingham equation were 25.7 per 1000 person years (25.0 to 26.3) for women and 26.4 (26.0 to 26.8) for men). At the 20% threshold, the population identified by QRISK2 was at higher risk of a CV event than the population identified by the Framingham score.
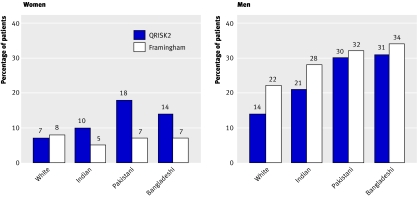
Conclusions: Incorporating ethnicity, deprivation, and other clinical conditions into the QRISK2 algorithm for risk of cardiovascular disease improves the accuracy of identification of those at high risk in a nationally representative population. At the 20% threshold, QRISK2 is likely to be a more efficient and equitable tool for treatment decisions for the primary prevention of cardiovascular disease. As the validation was performed in a similar population to the population from which the algorithm was derived, it potentially has a "home advantage." Further validation in other populations is therefore advised.
Conflict of interest statement
Competing interests: JR chaired and PB and RM were members of the NICE guideline development group on cardiovascular risk assessment. JHC is codirector of QRESEARCH—a not for profit organisation that is a joint partnership between the University of Nottingham and EMIS. EMIS is the leading commercial supplier of IT systems for 56% of general practices in England and Wales and it is likely to implement QRISK2 into its clinical management system. EMIS is likely to also distribute the software package for those using it for academic research or other organisations interesting in implementing QRISK2 into practice or (
Figures
Comment in
-
Cardiovascular risk tables.BMJ. 2008 Jun 28;336(7659):1445-6. doi: 10.1136/bmj.a480. Epub 2008 Jun 23. BMJ. 2008. PMID: 18573855 Free PMC article.
References
-
- British Heart Foundation. Coronary heart disease statistics London: British Heart Foundation, 2007
-
- North of England Hypertension Guideline Development Group. Essential hypertension: managing adult patients in primary care (NICE guideline) Newcastle, Centre for Health Services Research: University of Newcastle upon Tyne, 2004 - PubMed
-
- National Institute for Health and Clinical Excellence. Statins for the prevention of cardiovascular events in patients at increased risk of developing cardiovascular disease or those with established cardiovascular disease guidance London: NICE, 2006
-
- Department of Health. Putting prevention first: vascular checks: risk assessment and management London: DH, 2008:15.
-
- National Collaborating Centre for Primary Care. Section 4.3 of the guideline on cardiovascular risk assessment: the modification of blood lipids for the primary and secondary prevention of cardiovascular disease London: NICE, 2008:43.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical