

Defining the incidence of cardiorespiratory instability in patients in step-down units using an electronic integrated monitoring system
- PMID: 18574087
- PMCID: PMC3668698
- DOI: 10.1001/archinte.168.12.1300
Defining the incidence of cardiorespiratory instability in patients in step-down units using an electronic integrated monitoring system
Abstract
Background: To our knowledge, detection of cardiorespiratory instability using noninvasive monitoring via electronic integrated monitoring systems (IMSs) in intermediate or step-down units (SDUs) has not been described. We undertook this study to characterize respiratory status in an SDU population, to define features of cardiorespiratory instability, and to evaluate an IMS index value that should trigger medical emergency team (MET) activation.
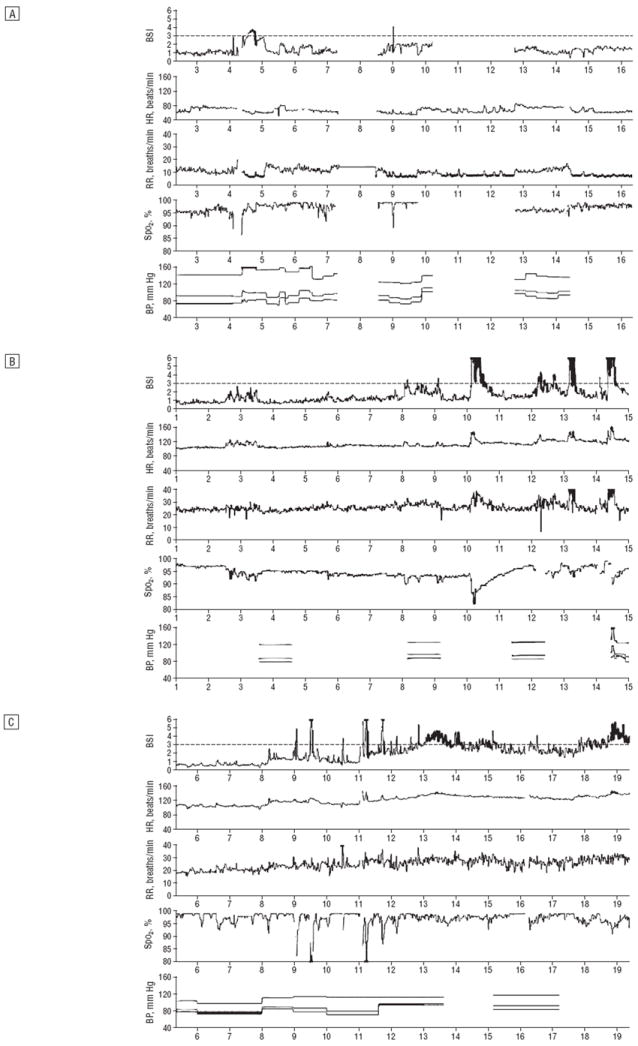
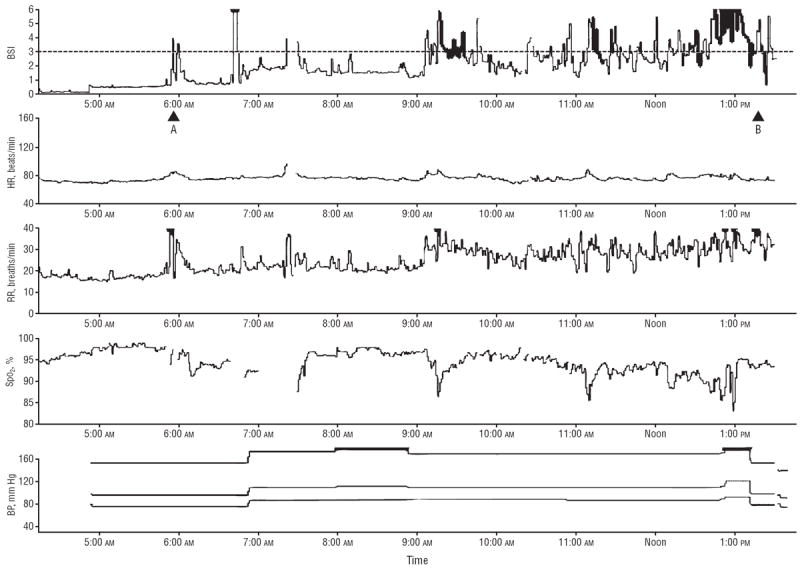
Methods: This descriptive, prospective, single-blinded, observational study evaluated all patients in a 24-bed SDU in a university medical center during 8 weeks from November 16, 2006, to January 11, 2007. An IMS (BioSign; OBS Medical, Carmel, Indiana) was inserted into the standard noninvasive hardwired monitoring system and used heart rate, blood pressure, respiratory rate, and peripheral oxygen saturation by pulse oximetry to develop a single neural networked signal, or BioSign Index (BSI). Data were analyzed for cardiorespiratory instability according to BSI trigger value and local MET activation criteria. Staff were blinded to BSI data collected in 326 patients (total census).
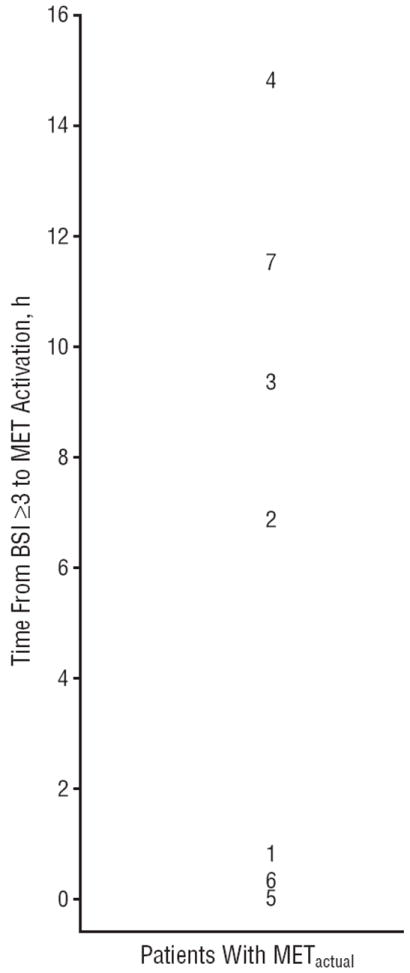
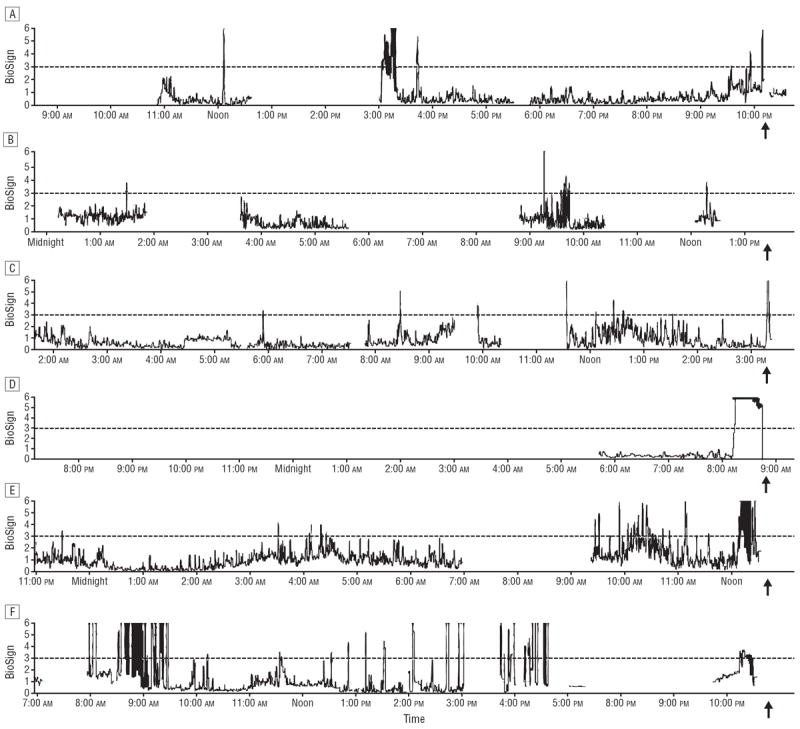
Results: Data for 18 248 hours of continuous monitoring were captured. Data for peripheral oxygen saturation by pulse oximetry were absent in 30% of monitored hours despite being a standard of care. Cardiorespiratory status in most patients (243 of 326 [74.5%]) was stable throughout their SDU stay, and instability in the remaining patients (83 of 326 [25%]) was exhibited infrequently. We recorded 111 MET activation criteria events caused by cardiorespiratory instability in 59 patients, but MET activation for this cause occurred in only 7 patients. All MET events were detected by BSI in advance (mean, 6.3 hours) in a bimodal distribution (>6 hours and < or =45 minutes).
Conclusions: Cardiorespiratory instability, while uncommon and often unrecognized, was preceded by elevation of the IMS index. Continuous noninvasive monitoring augmented by IMS provides sensitive detection of early instability in patients in SDUs.
Figures
Comment in
-
Integrated monitoring systems and patient safety: a need for further study.Arch Intern Med. 2008 Dec 8;168(22):2404. doi: 10.1001/archinte.168.22.2404. Arch Intern Med. 2008. PMID: 19064821 No abstract available.
References
-
- Devita MA, Bellomo R, Hillman K, et al. Findings of the first consensus conference on medical emergency teams. Crit Care Med. 2006;34(9):2463–2478. published correction appears in Crit Care Med. 2006;34(12):3070. - PubMed
-
- Subbe CP, Gao H, Harrison DA. Reproducibility of physiological track-and-trigger warning systems for identifying at-risk patients on the ward. Intensive Care Med. 2007;33(4):619–624. - PubMed
-
- Subbe CP, Kruger M, Rutherford P, Gemmel L. Validation of a modified Early Warning Score in medical admissions. Q J Med. 2001;94(10):521–526. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
