

Inflammation-associated insulin resistance: differential effects in rheumatoid arthritis and systemic lupus erythematosus define potential mechanisms
- PMID: 18576352
- PMCID: PMC2755593
- DOI: 10.1002/art.23600
Inflammation-associated insulin resistance: differential effects in rheumatoid arthritis and systemic lupus erythematosus define potential mechanisms
Abstract
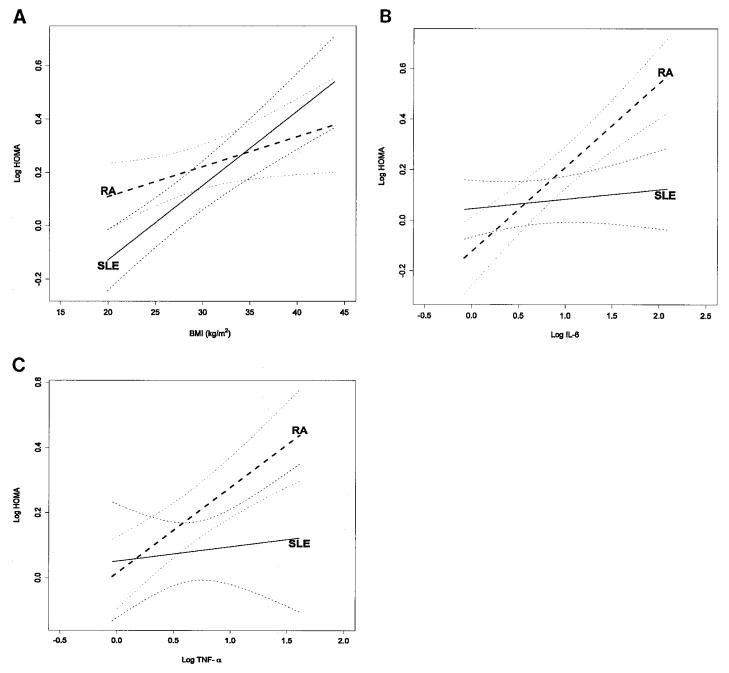
Objective: Insulin resistance is increased by inflammation, but the mechanisms are unclear. The present study was undertaken to test the hypothesis that decreased insulin sensitivity is differentially associated with mediators of inflammation by studying 2 chronic inflammatory diseases of different pathogenesis, systemic lupus erythematosus (SLE) and rheumatoid arthritis (RA).
Methods: We measured fasting insulin, glucose, and lipid levels, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), interleukin-6 (IL-6), tumor necrosis factor alpha (TNFalpha), and coronary artery calcification in 103 patients with SLE and in 124 patients with RA. Insulin sensitivity was measured using the homeostasis model assessment (HOMA) index.
Results: The HOMA value was higher in RA patients (median 2.05 [interquartile range (IQR) 1.05-3.54]) than in SLE patients (1.40 [0.78-2.59]) (P = 0.007). CRP and ESR did not differ significantly in RA and SLE patients. Body mass index (BMI) was significantly correlated with the HOMA index in both RA (rho = 0.20) and SLE (rho = 0.54), independently of age, sex, race, and current use of corticosteroids. In RA patients, the HOMA index was also significantly positively correlated with IL-6 (rho = 0.63), TNFalpha (rho = 0.50), CRP (rho = 0.29), ESR (rho = 0.26), coronary calcification (rho = 0.26), and Disease Activity Score in 28 joints (rho = 0.21); associations adjusted for age, sex, race, BMI, and current use of corticosteroids remained significant (P < 0.05). In SLE patients, the HOMA index was also significantly correlated with ESR (rho = 0.35) and CRP (rho = 0.25), but not with other variables. The association between the ESR and the HOMA value in patients with SLE remained significant after adjustment for confounding covariates (P = 0.008). In multivariable models, the major contributing factors to the HOMA index were the BMI in SLE patients, and IL-6 and TNFalpha levels in RA patients.
Conclusion: The pathogenesis of insulin resistance and its contribution to atherogenesis varies in different inflammatory settings.
Figures
References
-
- Chung CP, Oeser A, Solus JF, Avalos I, Gebretsadik T, Shintani A, et al. Prevalence of the metabolic syndrome is increased in rheumatoid arthritis and is associated with coronary atherosclerosis. Atherosclerosis. 2008;196:756–63. - PubMed
-
- Dessein PH, Joffe BI, Stanwix AE. Inflammation, insulin resistance, and aberrant lipid metabolism as cardiovascular risk factors in rheumatoid arthritis. J Rheumatol. 2003;30:1403–5. - PubMed
-
- El Magadmi M, Ahmad Y, Turkie W, Yates AP, Sheikh N, Bernstein RM, et al. Hyperinsulinemia, insulin resistance, and circulating oxidized low density lipoprotein in women with systemic lupus erythematosus. J Rheumatol. 2006;33:50–6. - PubMed
-
- Bray GA. Medical consequences of obesity. J Clin Endocrinol Metab. 2004;89:2583–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
