Point of care testing to improve glycemic control
- PMID: 18578216
- PMCID: PMC3782994
- DOI: 10.1108/09526860810868256
Point of care testing to improve glycemic control
Abstract
Purpose: The purpose of this paper is to pilot-test the feasibility and impact of protocol-driven point-of-care HbAlc testing on levels of glycemic control and on rates of diabetic regimen intensification in an urban community health center serving low-income patients.
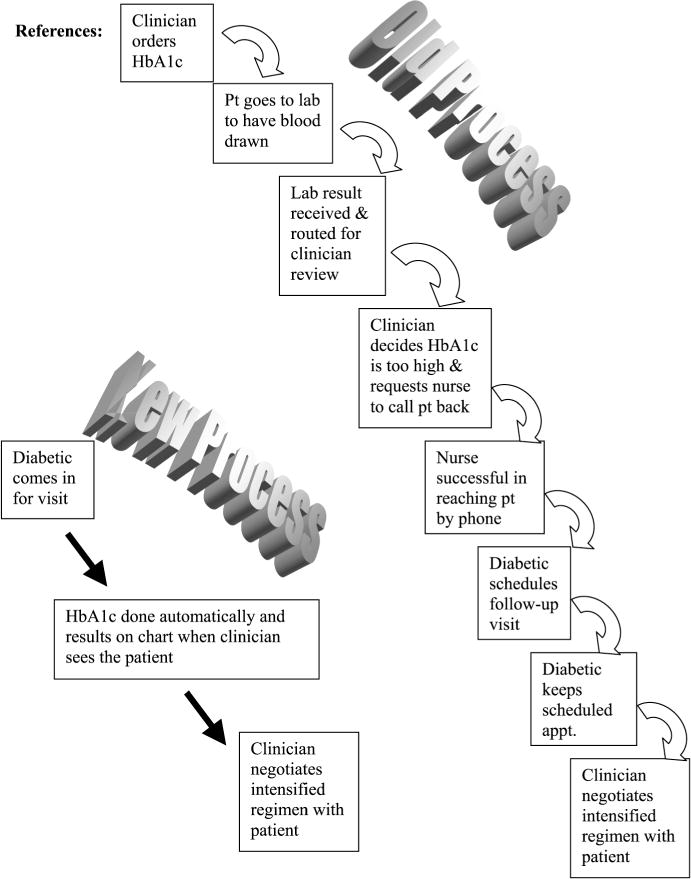
Design/methodology/approach: The paper suggests a primary care process re-design, using point of care finger-stick HbA1c testing under a standing order protocol that provided test results to the provider at patient visit.
Findings: The paper finds that the protocol was well received by both nurses and physicians. HbA1c testing rates increased from 73.6 percent to 86.8 percent (p = 0.40, n = 106). For the 69 patients who had both pre- and post-intervention results, HbAlc levels decreased significantly from 8.55 to 7.84 (p = 0.004, n = 69). At baseline, the health center as a system was relatively ineffective in responding to elevated HbA1c levels. An opportunity to intensify, i.e. a face-to-face visit with lab results available, occurred for only 68.6 percent of elevated HbAlc levels before the intervention, vs. 100 percent post-intervention (p < 0.001). Only 28.6 percent of patients with HbAlc levels >8.0 had their regimens intensified in the pre-intervention phase, compared with 53.8 percent in the post-intervention phase (p = 0.03).
Research limitations/implications: This was a pilot-study in one urban health center. Larger group-randomized controlled trials are needed.
Practical implications: The health center's performance as a system, improved significantly as a way of intensifying diabetic regimens thereby achieving improved glycemic control.
Originality/value: This intervention is feasible, replicable and scalable and does not rely on changing physician behaviors to improve primary care diabetic outcomes.
Figures
References
-
- Allsworth JE, Toppa R, Palin NC, Lapane KL. Racial and ethnic disparities in the pharmacologic management of diabetes mellitus among long-term care facility residents. Ethnicity and Disease. 2005;15(2):205–12. - PubMed
-
- Barnes CS, Ziemer DC, Miller CD, Doyle JP, Watkins C, Jr, Cook CB, Gallina DL, El-Kebbi I, Branch WT, Jr, Phillips LS. Little time for diabetes management in the primary care setting. Diabetes Education. 2004;30(1):126–35. - PubMed
-
- Belfiglio M, De Berardis G, Franciosi M, Cavaliere D, Di Nardo B, Greenfield S, Kaplan SH, Pellegrini F, Sacco M, Tognoni G, Valentini M, Nicolucci A, Caimi V, Capani F, Corsi A, Della Vedova R, Massi Benedetti M, Nicolucci A, Taboga C, Tombesi M, Vespasiani G. QuED Study Group – quality of care and outcomes in type 2 diabetes. The relationship between physicians’ self-reported target fasting blood glucose levels and metabolic control in type 2 diabetes. Diabetes Care. 2001;24(3):423–9. - PubMed
-
- Bernard AM, Anderson L, Cook CB, Phillips LS. What do internal medicine residents need to enhance their diabetes care? Diabetes Care. 1999;22(5):661–6. - PubMed
-
- Bodenheimer T, Wagner EH, Grumbach K. Improving primary care for patients with chronic illness: the chronic care model, part 2. Journal of the American Medical Association. 2002;288(15):1909–14. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous