

Effects of Glasgow Outcome Scale misclassification on traumatic brain injury clinical trials
- PMID: 18578634
- PMCID: PMC2946877
- DOI: 10.1089/neu.2007.0510
Effects of Glasgow Outcome Scale misclassification on traumatic brain injury clinical trials
Abstract
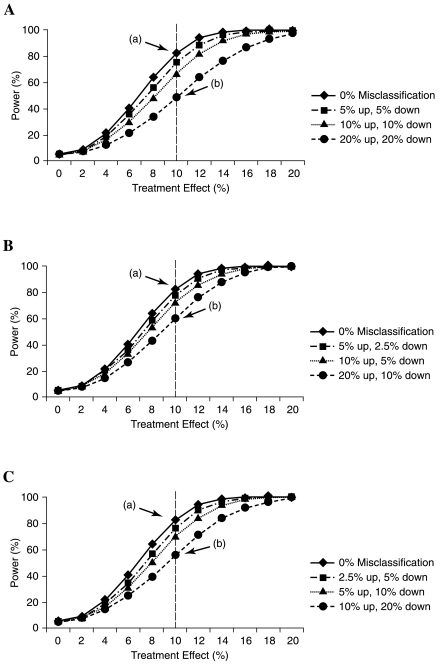
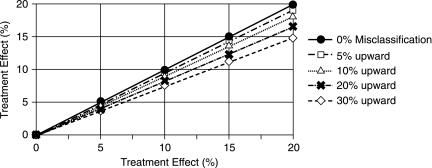
The Glasgow Outcome Scale (GOS) is the primary endpoint for efficacy analysis of clinical trials in traumatic brain injury (TBI). Accurate and consistent assessment of outcome after TBI is essential to the evaluation of treatment results, particularly in the context of multicenter studies and trials. The inconsistent measurement or interobserver variation on GOS outcome, or for that matter, on any outcome scales, may adversely affect the sensitivity to detect treatment effects in clinical trial. The objective of this study is to examine effects of nondifferential misclassification of the widely used five-category GOS outcome scale and in particular to assess the impact of this misclassification on detecting a treatment effect and statistical power. We followed two approaches. First, outcome differences were analyzed before and after correction for misclassification using a dataset of 860 patients with severe brain injury randomly sampled from two TBI trials with known differences in outcome. Second, the effects of misclassification on outcome distribution and statistical power were analyzed in simulation studies on a hypothetical 800-patient dataset. Three potential patterns of nondifferential misclassification (random, upward and downward) on the dichotomous GOS outcome were analyzed, and the power of finding treatments differences was investigated in detail. All three patterns of misclassification reduce the power of detecting the true treatment effect and therefore lead to a reduced estimation of the true efficacy. The magnitude of such influence not only depends on the size of the misclassification, but also on the magnitude of the treatment effect. In conclusion, nondifferential misclassification directly reduces the power of finding the true treatment effect. An awareness of this procedural error and methods to reduce misclassification should be incorporated in TBI clinical trials.
Figures
References
-
- Anderson S.I. Housley A.M. Jones P.A. Slattery J. Miller J.D. Glasgow Outcome Scale: an inter-rater reliability study. Brain Inj. 1993;7:309–317. - PubMed
-
- Bolland K. Sooriyarachchi M.R. Whitehead J. Sample size review in a head injury trial with ordered categorical responses. Statist. Med. 1998;17:2835–2847. - PubMed
-
- Bullock M.R. Merchant R.E. Choi S.C. Gilman C.B. Kreutzer J.S. Marmarou A. Teasdale G.M. Outcome measures for clinical trials in neurotrauma. Neurosurg. Focus. 2002;13:ECP1. - PubMed
-
- Choi S.C. Clifton G.L. Marmarou A. Miller E.R. Misclassification and treatment effect on primary outcome measures in clinical trials of severe neurotrauma. J. Neurotrauma. 2002;19:17–22. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
