

Angiotensin II blockade and aortic-root dilation in Marfan's syndrome
- PMID: 18579813
- PMCID: PMC2692965
- DOI: 10.1056/NEJMoa0706585
Angiotensin II blockade and aortic-root dilation in Marfan's syndrome
Abstract
Background: Progressive enlargement of the aortic root, leading to dissection, is the main cause of premature death in patients with Marfan's syndrome. Recent data from mouse models of Marfan's syndrome suggest that aortic-root enlargement is caused by excessive signaling by transforming growth factor beta (TGF-beta) that can be mitigated by treatment with TGF-beta antagonists, including angiotensin II-receptor blockers (ARBs). We evaluated the clinical response to ARBs in pediatric patients with Marfan's syndrome who had severe aortic-root enlargement.
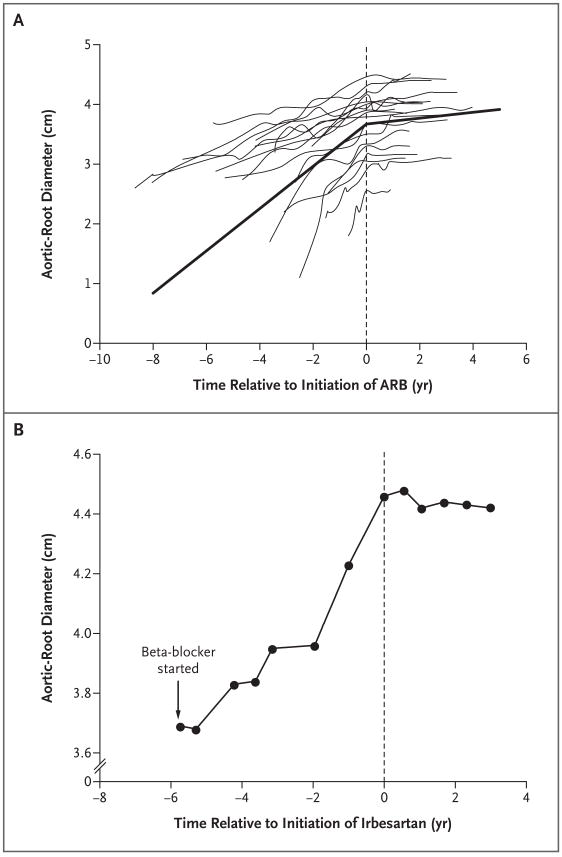
Methods: We identified 18 pediatric patients with Marfan's syndrome who had been followed during 12 to 47 months of therapy with ARBs after other medical therapy had failed to prevent progressive aortic-root enlargement. The ARB was losartan in 17 patients and irbesartan in 1 patient. We evaluated the efficacy of ARB therapy by comparing the rates of change in aortic-root diameter before and after the initiation of treatment with ARBs.
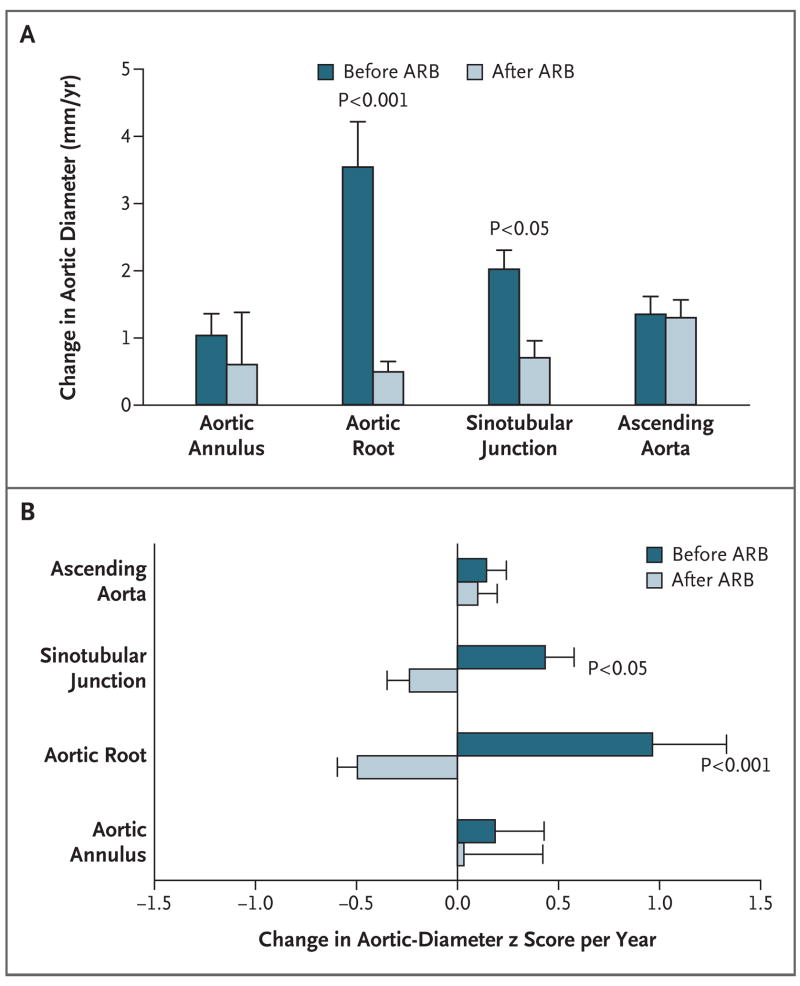
Results: The mean (+/-SD) rate of change in aortic-root diameter decreased significantly from 3.54+/-2.87 mm per year during previous medical therapy to 0.46+/-0.62 mm per year during ARB therapy (P<0.001). The deviation of aortic-root enlargement from normal, as expressed by the rate of change in z scores, was reduced by a mean difference of 1.47 z scores per year (95% confidence interval, 0.70 to 2.24; P<0.001) after the initiation of ARB therapy. The sinotubular junction, which is prone to dilation in Marfan's syndrome as well, also showed a reduced rate of change in diameter during ARB therapy (P<0.05), whereas the distal ascending aorta, which does not normally become dilated in Marfan's syndrome, was not affected by ARB therapy.
Conclusions: In a small cohort study, the use of ARB therapy in patients with Marfan's syndrome significantly slowed the rate of progressive aortic-root dilation. These findings require confirmation in a randomized trial.
2008 Massachusetts Medical Society
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
A small molecule for a large disease.N Engl J Med. 2008 Jun 26;358(26):2829-31. doi: 10.1056/NEJMe0804008. N Engl J Med. 2008. PMID: 18579819 No abstract available.
-
Angiotensin II blockade in Marfan's syndrome.N Engl J Med. 2008 Oct 16;359(16):1732; author reply 1733-4. doi: 10.1056/NEJMc081528. N Engl J Med. 2008. Retraction in: N Engl J Med. 2015 Dec 3;373(23):2280. doi: 10.1056/NEJMe1514259. PMID: 18923178 Retracted. No abstract available.
-
Angiotensin II blockade in Marfan's syndrome.N Engl J Med. 2008 Oct 16;359(16):1732-3; author reply 1733-4. N Engl J Med. 2008. PMID: 18927953 No abstract available.
-
Angiotensin II blockade in Marfan's syndrome.N Engl J Med. 2008 Oct 16;359(16):1733; author reply 1733-4. N Engl J Med. 2008. PMID: 18927954 No abstract available.
References
-
- Dietz HC, Cutting GR, Pyeritz RE, et al. Marfan syndrome caused by a recurrent de novo missense mutation in the fibrillin gene. Nature. 1991;352:337–9. - PubMed
-
- Dietz HC, Pyeritz RE. Mutations in the human gene for fibrillin-1 (FBN1) in the Marfan syndrome and related disorders. Hum Mol Genet. 1995;4:1799–809. - PubMed
-
- Milewicz DM, Dietz HC, Miller DC. Treatment of aortic disease in patients with Marfan syndrome. Circulation. 2005;111(11):e150–e157. - PubMed
-
- Shores J, Berger KR, Murphy EA, Pyeritz RE. Progression of aortic dilatation and the benefit of long-term β-adrenergic blockade in Marfan’s syndrome. N Engl J Med. 1994;330:1335–41. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical