

Prediction of the survival and functional ability of severe stroke patients after ICU therapeutic intervention
- PMID: 18582387
- PMCID: PMC2443378
- DOI: 10.1186/1471-2377-8-24
Prediction of the survival and functional ability of severe stroke patients after ICU therapeutic intervention
Abstract
Background: This study evaluated the benefits and impact of ICU therapeutic interventions on the survival and functional ability of severe cerebrovascular accident (CVA) patients.
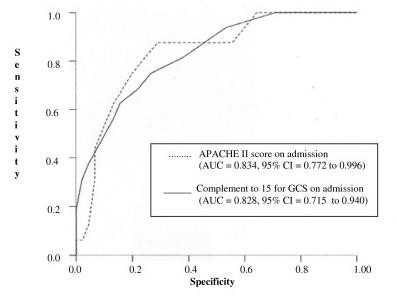
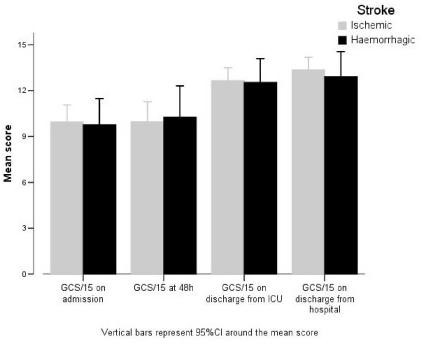
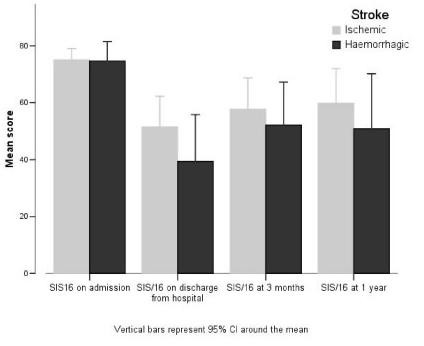
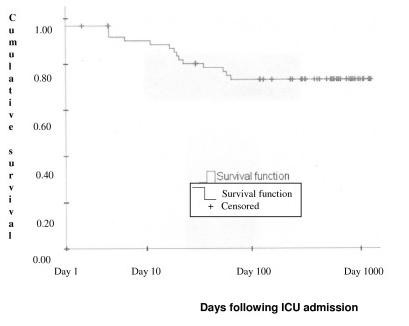
Methods: Sixty-two ICU patients suffering from severe ischemic/haemorrhagic stroke were evaluated for CVA severity using APACHE II and the Glasgow coma scale (GCS). Survival was determined using Kaplan-Meier survival tables and survival prediction factors were determined by Cox multivariate analysis. Functional ability was assessed using the stroke impact scale (SIS-16) and Karnofsky score. Risk factors, life support techniques and neurosurgical interventions were recorded. One year post-CVA dependency was investigated using multivariate analysis based on linear regression.
Results: The study cohort constituted 6% of all CVA (37.8% haemorrhagic/62.2% ischemic) admissions. Patient mean(SD) age was 65.8(12.3) years with a 1:1 male: female ratio. During the study period 16 patients had died within the ICU and seven in the year following hospital release. The mean(SD) APACHE II score at hospital admission was 14.9(6.0) and ICU mean duration of stay was 11.2(15.4) days. Mechanical ventilation was required in 37.1% of cases. Risk ratios were; GCS at admission 0.8(0.14), (p = 0.024), APACHE II 1.11(0.11), (p = 0.05) and duration of mechanical ventilation 1.07(0.07), (p = 0.046). Linear coefficients were: type of CVA - haemorrhagic versus ischemic: -18.95(4.58) (p = 0.007), GCS at hospital admission: -6.83(1.08), (p = 0.001), and duration of hospital stay -0.38(0.14), (p = 0.40).
Conclusion: To ensure a better prognosis CVA patients require ICU therapeutic interventions. However, as we have shown, where tests can determine the worst affected patients with a poor vital and functional outcome should treatment be withheld?
Figures
Similar articles
-
Acute physiology and chronic health evaluation (APACHE II) and Glasgow coma scores as predictors of outcome from intensive care after cardiac arrest.Crit Care Med. 1991 Dec;19(12):1465-73. doi: 10.1097/00003246-199112000-00005. Crit Care Med. 1991. PMID: 1959364 Clinical Trial.
-
Clinical Predictors of Survival and Functional Outcome of Stroke Patients Admitted to Critical Care.Crit Care Med. 2018 Jul;46(7):1085-1092. doi: 10.1097/CCM.0000000000003127. Crit Care Med. 2018. PMID: 29608513
-
Comparison of the APACHE III, APACHE II and Glasgow Coma Scale in acute head injury for prediction of mortality and functional outcome.Intensive Care Med. 1997 Jan;23(1):77-84. doi: 10.1007/s001340050294. Intensive Care Med. 1997. PMID: 9037644
-
Admission to a neurologic/neurosurgical intensive care unit is associated with reduced mortality rate after intracerebral hemorrhage.Crit Care Med. 2001 Mar;29(3):635-40. doi: 10.1097/00003246-200103000-00031. Crit Care Med. 2001. PMID: 11373434
-
Stroke Is Not an Accident: An Integrative Review on the Use of the Term Cerebrovascular Accident.Neuroepidemiology. 2024 Oct 28:1-9. doi: 10.1159/000542301. Online ahead of print. Neuroepidemiology. 2024. PMID: 39467531 Review.
Cited by
-
Characteristics and outcome of stroke patients with cerebrovascular accident at the intensive care unit of a tertiary hospital in Nigeria.J West Afr Coll Surg. 2013 Jan;3(1):1-13. J West Afr Coll Surg. 2013. PMID: 25453008 Free PMC article.
-
The epidemiology of stroke in the Middle East.Eur Stroke J. 2016 Sep;1(3):180-198. doi: 10.1177/2396987316654338. Epub 2016 Jun 28. Eur Stroke J. 2016. PMID: 31008279 Free PMC article. Review.
-
Anxiety and depression one year after the first stroke among Lebanese survivors: proportions, changes, and predictors.BMC Psychiatry. 2025 May 31;25(1):558. doi: 10.1186/s12888-025-06997-9. BMC Psychiatry. 2025. PMID: 40450195 Free PMC article.
-
Predicting recovery of voluntary upper extremity movement in subacute stroke patients with severe upper extremity paresis.PLoS One. 2015 May 14;10(5):e0126857. doi: 10.1371/journal.pone.0126857. eCollection 2015. PLoS One. 2015. PMID: 25973919 Free PMC article.
-
Outcomes of patients admitted to the ICU for acute stroke: a retrospective cohort.BMC Anesthesiol. 2022 Jul 25;22(1):235. doi: 10.1186/s12871-022-01777-4. BMC Anesthesiol. 2022. PMID: 35879652 Free PMC article.
References
-
- How do stroke units improve patient outcomes? A collaborative systematic review of the randomized trials. Stroke Unit Trialists Collaboration. Stroke. 1997;28:2139–44. - PubMed
-
- Indredavik B, Slordahl SA, Bakke F, Rokseth R, Haheim LL. Stroke unit treatment. Long-term effects. Stroke. 1997;28:1861–6. - PubMed
-
- Denicourt C, Dowdy SF. Protein transduction technology offers novel therapeutic approach for brain ischemia. Trends Pharmacol Sci. 2003;24:216–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
