

Stability of intracranial aneurysms adequately occluded 6 months after coiling: a 3T MR angiography multicenter long-term follow-up study
- PMID: 18583406
- PMCID: PMC8118778
- DOI: 10.3174/ajnr.A1181
Stability of intracranial aneurysms adequately occluded 6 months after coiling: a 3T MR angiography multicenter long-term follow-up study
Abstract
Background and purpose: The long-term fate of coiled intracranial aneurysms is largely unknown, and prolonged imaging follow-up has been advocated. The yield of follow-up imaging in coiled aneurysms adequately occluded at 6 months is unknown. In such patients, we performed time-of-flight MR angiography (MRA) to assess the incidence and therapeutic consequences of reopening 5-11 years after coiling.
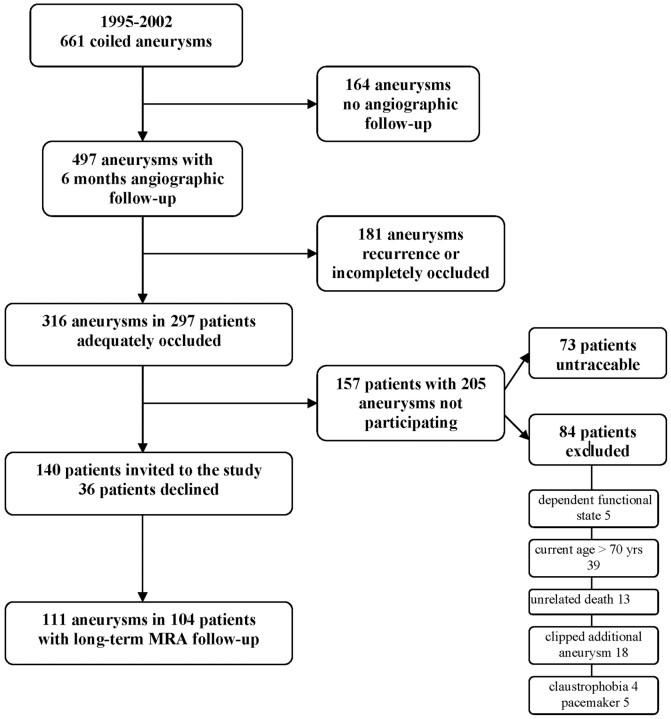
Materials and methods: Between 1995 and 2002, 661 aneurysms in 607 patients were coiled in 3 participating centers. Six-month follow-up angiograms were obtained in 497 (75%) aneurysms, of which 316 (64%) in 297 patients were adequately occluded. Of 297 patients, 84 were excluded for various reasons and 73 could not be traced. Of 140 eligible patients, 104 (74%) with 111 aneurysms were studied with 3T MR imaging and high-resolution MRA at a mean of 6.0 years after coiling (median, 5.6 years; range, 5.0-10.6 years).
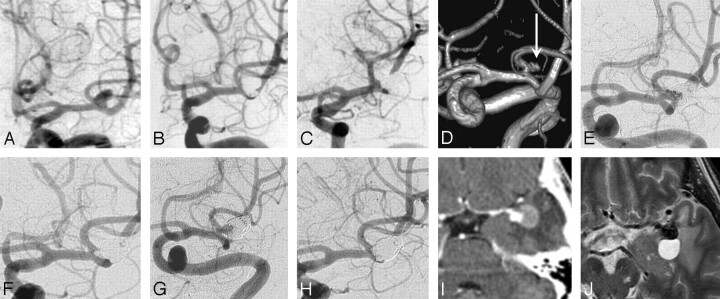
Results: The proportion of aneurysms with reopening was 3.6% (4/111; 95% confidence interval [CI], 1.1%-9.2%). One reopened aneurysm, which initially contained intraluminal thrombus, was additionally coiled (0.9%; 95% CI, 0.0%-5.4%).
Conclusion: In intracranial aneurysms with adequate occlusion at 6 months after coiling, the proportion of reopening needing retreatment after >5 years is low. The number of reopened aneurysms with therapeutic consequences was too small to assess risk factors, but probably the presence of intraluminal thrombus is one such risk factor. Most patients with coiled intracranial aneurysms that are adequately occluded at 6 months might not need prolonged imaging follow-up.
Figures
References
-
- Molyneux AJ, Kerr RS, Yu LM, et al. International Subarachnoid Aneurysm Trial (ISAT) Collaborative Group: International Subarachnoid Aneurysm Trial (ISAT) of neurosurgical clipping versus endovascular coiling in 2143 patients with ruptured intracranial aneurysms—a randomised trial. Lancet 2002;360:1267–74 - PubMed
-
- Brilstra EH, Rinkel GJ, van der Graaf Y, et al. Treatment of intracranial aneurysms by embolization with coils: a systematic review. Stroke 1999;30:470–76 - PubMed
-
- Sluzewski M, van Rooij WJ, Rinkel GJ, et al. Endovascular treatment of ruptured intracranial aneurysms with detachable coils: long-term clinical and serial angiographic results. Radiology 2003;227:720–24 - PubMed
-
- Cognard C, Weill A, Spelle L, et al. Long-term angiographic follow-up of 169 intracranial aneurysms occluded with detachable coils. Radiology 1999;212:348–56 - PubMed
-
- Raymond J, Guilbert F, Weill A, et al. Long-term angiographic recurrences after selective endovascular treatment of aneurysms with detachable coils. Stroke 2003;34:1398–403 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical