

Prevalence and correlates of silent cerebral infarcts in the Framingham offspring study
- PMID: 18583555
- PMCID: PMC2712254
- DOI: 10.1161/STROKEAHA.108.516575
Prevalence and correlates of silent cerebral infarcts in the Framingham offspring study
Abstract
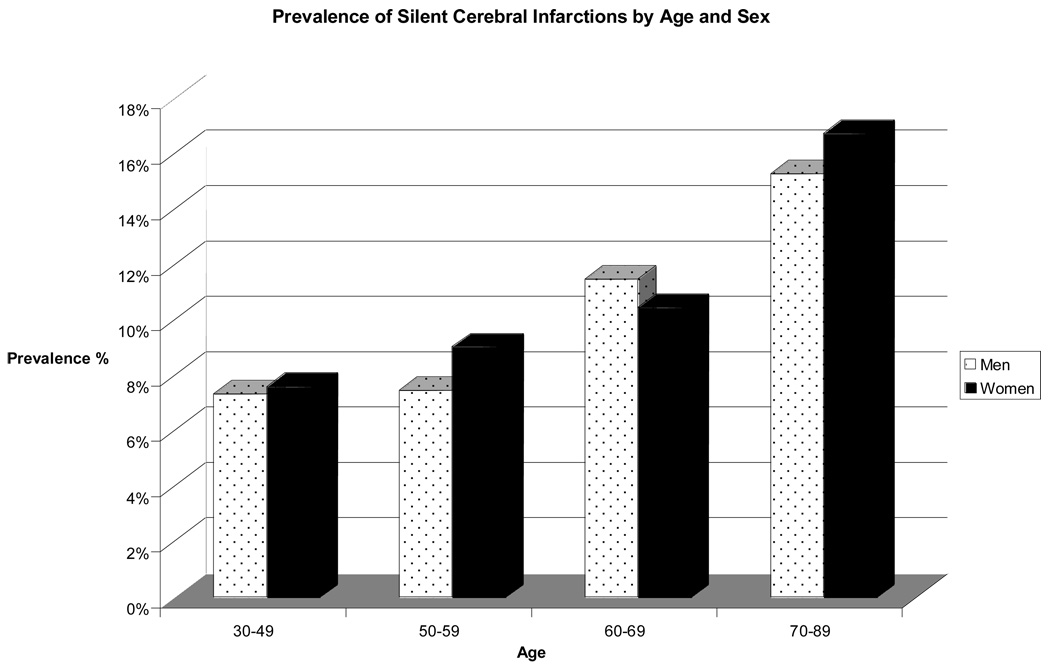
Background and purpose: Previous estimates of the prevalence of silent cerebral infarction (SCI) on MRI in community-based samples have varied between 5.8% and 17.7% depending on age, ethnicity, presence of comorbidities, and imaging techniques. We document the prevalence and risk factors associated with SCI at midlife in the community-based Framingham sample.
Methods: Our study sample comprised 2040 Framingham Offspring (53% female; mean age, 62+/-9 years) who attended the sixth examination (1996-1998), underwent volumetric brain MRI (1999-2005,) and were free of clinical stroke at MRI. We examined the age- and sex-specific prevalences and the clinical correlates of SCI using multivariable logistic regression models.
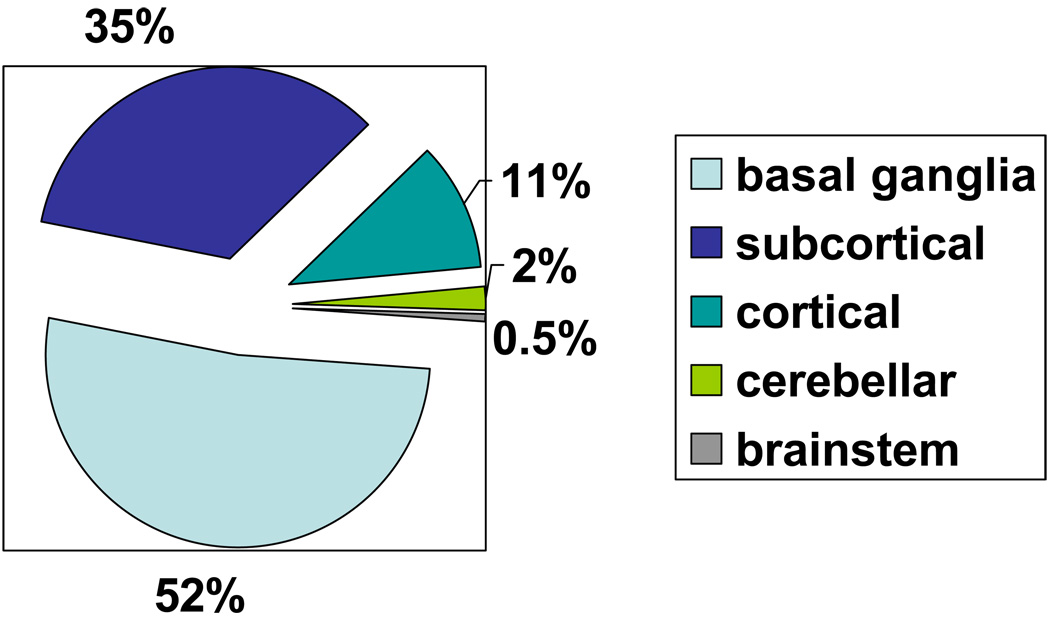
Results: At least 1 SCI was present in 10.7% of participants; 84% had a single lesion. SCI was largely located in the basal ganglia (52%), other subcortical (35%) areas, and cortical areas (11%). Prevalent SCI was associated with the Framingham Stroke Risk Profile score (OR, 1.27; 95% CI, 1.10-1.46); stage I hypertension was determined by JNC-7 criteria (OR,1.56; CI,1.15-2.11), an elevated plasma homocysteine in the highest quartile (OR, 2.23; CI, 1.42-3.51), atrial fibrillation (OR, 2.16; CI, 1.07-4.40), carotid stenosis >25% (OR, 1.62; 1.13-2.34), and increased carotid intimal-medial thickness above the lowest quintile (OR, 1.65; CI, 1.22-2.24).
Conclusions: The prevalence and distribution of SCI in the Framingham Offspring are comparable to previous estimates. Risk factors previously associated with clinical stroke were also found to be associated with midlife SCI. Our results support current guidelines emphasizing early detection and treatment of stroke risk factors.
Figures
Comment in
-
Silent cerebral infarction: are we listening?Stroke. 2008 Nov;39(11):2919-20. doi: 10.1161/STROKEAHA.108.523803. Epub 2008 Jun 26. Stroke. 2008. PMID: 18583550 No abstract available.
References
-
- Masuda J, Nabika T, Notsu Y. Silent stroke: Pathogenesis, genetic factors and clinical implications as a risk factor. Curr Opin Neurol. 2001;14:77–82. - PubMed
-
- Fisher CM. Lacunes: Small, deep cerebral infarcts. Neurology. 1965;15:774–784. - PubMed
-
- Lee SC, Park SJ, Ki HK, Gwon HC, Chung CS, Byun HS, Shin KJ, Shin MH, Lee WR. Prevalence and risk factors of silent cerebral infarction in apparently normal adults. Hypertension. 2000;36:73–77. - PubMed
-
- Price TR, Manolio TA, Kronmal RA, Kittner SJ, Yue NC, Robbins J, Anton-Culver H, O'Leary DH. Silent brain infarction on magnetic resonance imaging and neurological abnormalities in community-dwelling older adults. The cardiovascular health study. Chs collaborative research group. Stroke. 1997;28:1158–1164. - PubMed
-
- Vermeer SE, Koudstaal PJ, Oudkerk M, Hofman A, Breteler MM. Prevalence and risk factors of silent brain infarcts in the population-based rotterdam scan study. Stroke. 2002;33:21–25. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
