

Cerebrovascular disease and stroke
- PMID: 18591185
- PMCID: PMC2677268
- DOI: 10.1136/adc.2008.142836
Cerebrovascular disease and stroke
Abstract
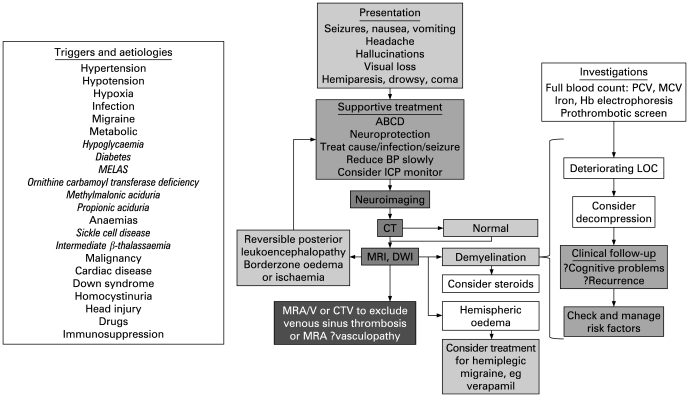
Stroke and cerebrovascular disorders are important causes of morbidity and mortality in children; they are already amongst the top 10 causes of childhood death and are probably increasing in prevalence. Acute treatment of stroke syndromes in adults is now evidence based. However, paediatric stroke syndromes are far less common and the differential diagnosis is very wide, but the individual health resource implications are much greater because of the life-long treatment costs in survivors. Recognition and consultation with a paediatric neurologist should be rapid so that children can benefit from regional services with emergency neurological, neuroradiological and neurosurgical intervention and paediatric intensive care. This review focuses on the epidemiology, presentation, differential diagnosis, generic/specific emergency management and prognosis of acute stroke in children. Its aim is to educate and guide management by general paediatricians and to emphasise the importance of local guidelines for the initial investigation and treatment and appropriate transfer of these children.
Conflict of interest statement
Figures
References
-
- Zahuranec DB, Brown DL, Lisabeth LD, et al. Is it time for a large, collaborative study of pediatric stroke? Stroke 2005;36:1825–9 - PubMed
-
- Telfer P, Coen P, Chakravorty S, et al. Clinical outcomes in children with sickle cell disease living in England: a neonatal cohort in East London. Haematologica 2007;92:905–12 - PubMed
-
- Mazumdar M, Heeney MM, Sox CM, et al. Preventing stroke among children with sickle cell anemia: an analysis of strategies that involve transcranial Doppler testing and chronic transfusion. Pediatrics 2007;120:e1107–16 - PubMed
-
- Laugesaar R, Kolk A, Tomberg T, et al. Acutely and retrospectively diagnosed perinatal stroke: a population-based study. Stroke 2007;38:2234–40 - PubMed
-
- Braun KP, Kappelle LJ, Kirkham FJ, et al. Diagnostic pitfalls in paediatric ischaemic stroke. Dev Med Child Neurol 2006;48:985–90 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources