

The effect of comorbid illness and functional status on the expected benefits of intensive glucose control in older patients with type 2 diabetes: a decision analysis
- PMID: 18591633
- PMCID: PMC2562733
- DOI: 10.7326/0003-4819-149-1-200807010-00005
The effect of comorbid illness and functional status on the expected benefits of intensive glucose control in older patients with type 2 diabetes: a decision analysis
Abstract
Background: Physicians are uncertain about when to pursue intensive glucose control among older patients with diabetes.
Objective: To assess the effect of comorbid illnesses and functional status, mediated through background mortality, on the expected benefits of intensive glucose control.
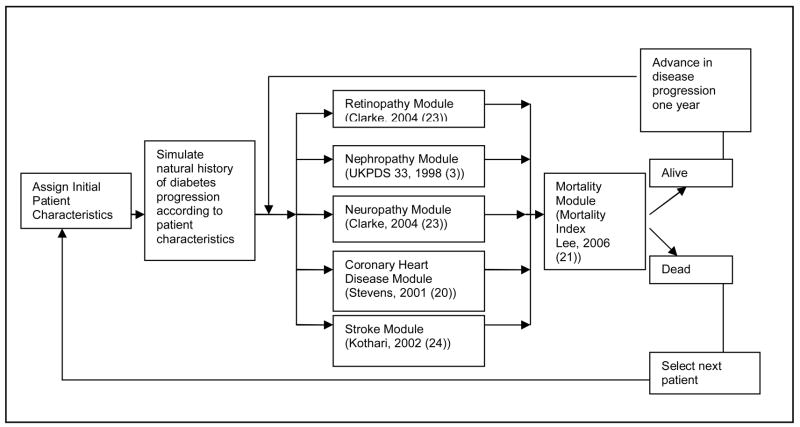
Design: Decision analysis.
Data sources: Major clinical studies in diabetes and geriatrics.
Target population: Patients 60 to 80 years of age who have type 2 diabetes and varied life expectancies estimated from a mortality index that was validated at the population level.
Time horizon: Patient lifetime.
Perspective: Health care system.
Intervention: Intensive glucose control (hemoglobin A1c [HbA1c] level of 7.0) versus moderate glucose control (HbA1c level of 7.9).
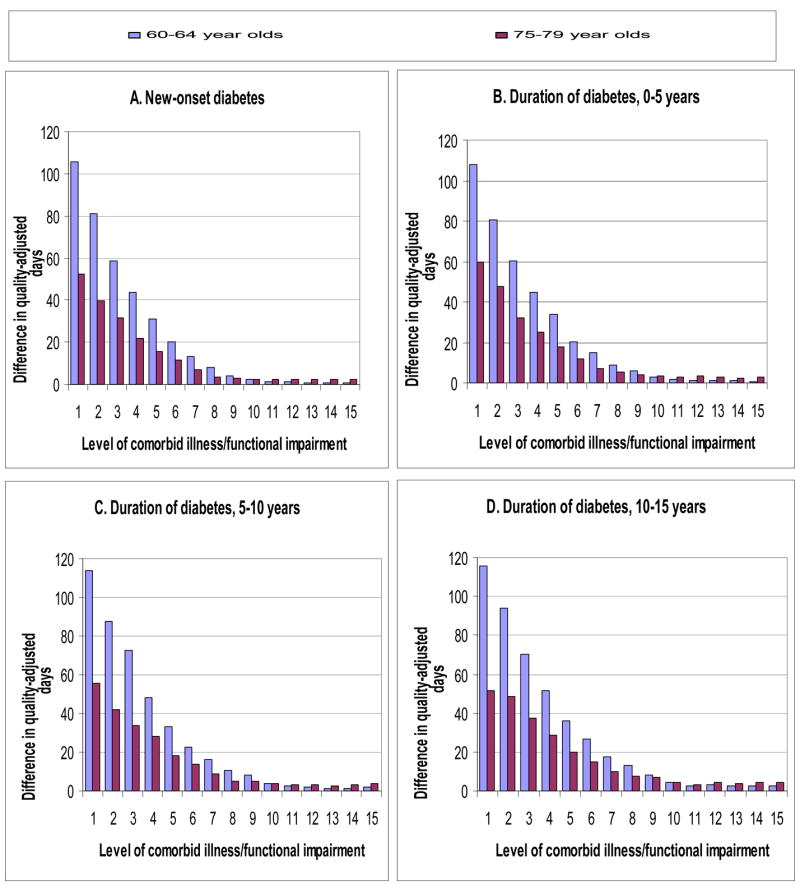
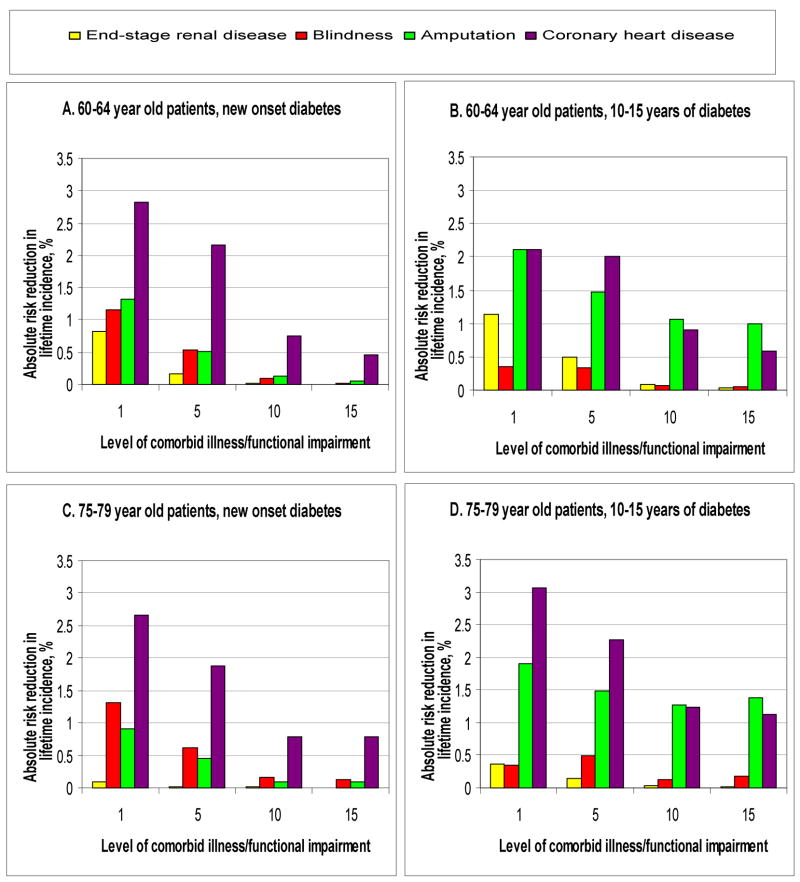
Outcome measures: Lifetime differences in incidence of complications and average quality-adjusted days.
Results of base-case analysis: Healthy older patients of different age groups had expected benefits of intensive glucose control ranging from 51 to 116 quality-adjusted days. Within each age group, the expected benefits of intensive control steadily declined as the level of comorbid illness and functional impairment increased (mortality index score, 1 to 26 points). For patients 60 to 64 years of age with new-onset diabetes, the benefits declined from 106 days at baseline good health (life expectancy, 14.6 years) to 44 days with 3 additional index points (life expectancy, 9.7 years) and 8 days with 7 additional index points (life expectancy, 4.8 years). A similar decline in benefits occurred among patients with prolonged duration of diabetes.
Results of sensitivity analysis: With alternative model assumptions (such as Framingham models), expected benefits of intensive control declined as mortality index scores increased.
Limitations: Diabetes clinical trial data were lacking for frail, older patients. The mortality index was not validated for use in predicting individual-level life expectancies. Adverse effects of intensive control were not taken into account.
Conclusion: Among older diabetic patients, the presence of multiple comorbid illnesses or functional impairments is a more important predictor of limited life expectancy and diminishing expected benefits of intensive glucose control than is age alone.
Figures
Comment in
-
Does comorbidity affect the benefit of intensive glycemic control in older patients with type 2 diabetes mellitus?Nat Clin Pract Endocrinol Metab. 2009 Feb;5(2):78-9. doi: 10.1038/ncpendmet1041. Epub 2008 Dec 17. Nat Clin Pract Endocrinol Metab. 2009. PMID: 19092787 No abstract available.
References
-
- American Diabetes Association. Standards of medical care in diabetes. Diabetes Care. 2005;28(Supplement 1):S4–S36. - PubMed
-
- The Diabetes Control and Complications Trial Research Group. The Effect Of Intensive Treatment Of Diabetes On The Development And Progression Of Long-Term Complications In Insulin-Dependent Diabetes Mellitus. N Engl J Med. 1993;329(14):977–986. - PubMed
-
- U. K. Prospective Diabetes Study Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) Lancet. 1998;352(9131):837–853. - PubMed
-
- Fleming BB, Greenfield S, Engelgau MM, et al. The diabetes quality improvement project. Diabetes Care. 2001;24(10):1815–1820. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials