

Anatomic Variations of the Sphenoid Sinus and Their Impact on Trans-sphenoid Pituitary Surgery
- PMID: 18592020
- PMCID: PMC2435468
- DOI: 10.1055/s-2007-992764
Anatomic Variations of the Sphenoid Sinus and Their Impact on Trans-sphenoid Pituitary Surgery
Abstract
Introduction: The trans-sphenoid access to the pituitary gland is becoming the most common approach for pituitary adenomas. Preoperative evaluation of the anatomy of the sphenoid sinus by computed tomography (CT) scan and magnetic resonance imaging (MRI) is a routine procedure and can direct the surgical decision.
Purpose: This work determines the incidence of the different anatomical variations of the sphenoid sinus as detected by MRI and CT scan and their impact on the approach.
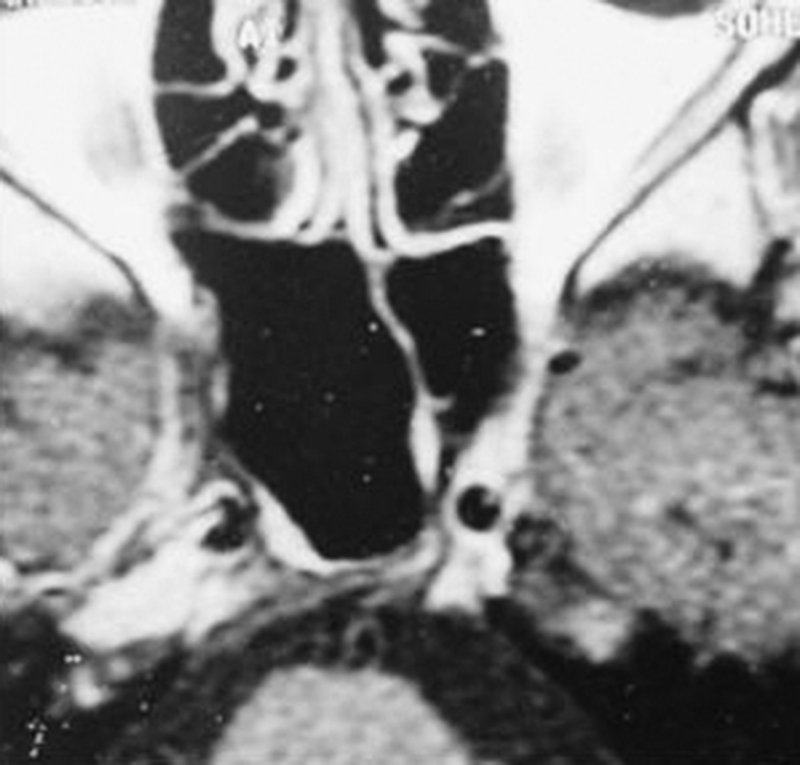
Methods: The CT scan and MRI of 296 patients operated for pituitary adenomas via a trans-sphenoid approach were retrospectively reviewed regarding the different anatomical variations of the sphenoid sinus: degree of pneumatization, sellar configuration, septation pattern, and the intercarotid distance.
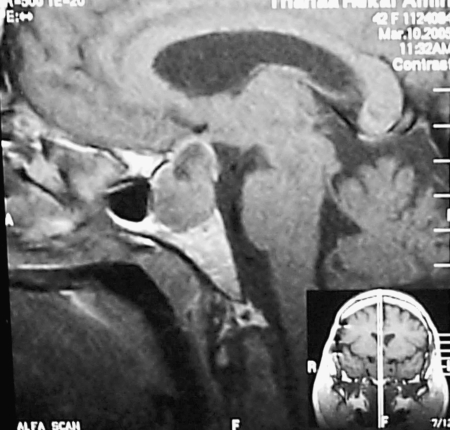
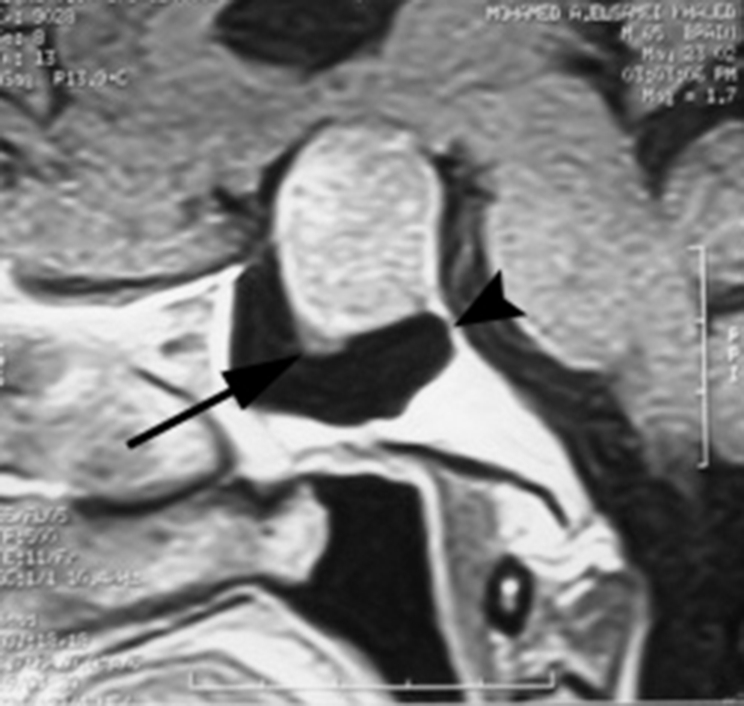
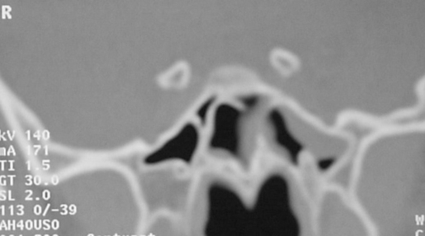
Results: There were 6 cases with conchal pneumatization, 62 patients with presellar, 162 patients with sellar, and 66 patients with postsellar pneumatization. There was sellar bulge in 232 patients, whereas this bulge was absent in 64 patients. There was no intersphenoid sinus septum in 32 patients, a single intersphenoid septum in 212 patients, and an accessory septum in 32 patients. Intraoperatively, the sellar bulge was marked in 189 cases and was mild in 43 cases.
Discussion: The pattern of pneumatization of the sphenoid sinus significantly affects the safe access to the sella. A highly pneumatized sphenoid sinus may distort the anatomic configuration, so in these cases it is extremely important to be aware of the midline when opening the sella to avoid accidental injury to the carotid and optic nerves. The sellar bulge is considered one of the most important surgical landmarks, facilitating the access to the sella. The surgical position of the patient is also a crucial point to avoid superior or posterior misdirection with resultant complications. It is wise to use extreme caution while removing the terminal septum.
Conclusion: Different anatomical configurations of the sphenoid sinus can seriously affect the access to the sella via the nose. The surgeon should be aware of these findings preoperatively to reach the sella safely and effectively.
Keywords: Sphenoid sinus; pituitary adenoma; pneumatization; trans-sphenoid approach.
Figures


Similar articles
-
Anatomical Variations of Sphenoid Sinus in South Indian Population: All That You Need for Trans-Sphenoidal Pituitary Surgery.Indian J Otolaryngol Head Neck Surg. 2022 Oct;74(Suppl 2):1646-1650. doi: 10.1007/s12070-021-02793-5. Epub 2021 Aug 3. Indian J Otolaryngol Head Neck Surg. 2022. PMID: 36452778 Free PMC article.
-
Dimensions, septation, and pattern of pneumatization of the sphenoidal sinus.Folia Morphol (Warsz). 2009 Nov;68(4):228-32. Folia Morphol (Warsz). 2009. PMID: 19950072
-
Prevalence of Anatomical Variations of Sphenoid Sinus and Its Adjacent Structures Pneumatization and Its Significance: A CT Scan Study.Indian J Otolaryngol Head Neck Surg. 2023 Dec;75(4):2979-2989. doi: 10.1007/s12070-023-03879-y. Epub 2023 Jun 2. Indian J Otolaryngol Head Neck Surg. 2023. PMID: 37974780 Free PMC article.
-
Is Complex Sphenoidal Sinus Anatomy a Contraindication to a Transsphenoidal Approach for Resection of Sellar Lesions? Case Series and Review of the Literature.World Neurosurg. 2017 Apr;100:173-179. doi: 10.1016/j.wneu.2016.12.123. Epub 2017 Jan 5. World Neurosurg. 2017. PMID: 28065874 Review.
-
Acromegaly due to an ectopic pituitary adenoma in the sphenoid sinus.Acta Radiol. 2004 Oct;45(6):689-91. doi: 10.1080/02841850410008405. Acta Radiol. 2004. PMID: 15587430 Review.
Cited by
-
Endoscopic anatomy of sellar region.Pituitary. 2013 Jun;16(2):251-9. doi: 10.1007/s11102-012-0413-9. Pituitary. 2013. PMID: 22847021
-
Eustachian tube communicating with sphenoid sinus: report of a novel anatomical variant.Surg Radiol Anat. 2017 Apr;39(4):461-465. doi: 10.1007/s00276-016-1740-8. Epub 2016 Sep 21. Surg Radiol Anat. 2017. PMID: 27650645 Review.
-
Anatomical Variations of the Nose and Paranasal Sinuses: A Computed Tomographic Study.Indian J Otolaryngol Head Neck Surg. 2019 Nov;71(Suppl 3):2231-2240. doi: 10.1007/s12070-019-01716-9. Epub 2019 Jul 26. Indian J Otolaryngol Head Neck Surg. 2019. PMID: 31763326 Free PMC article.
-
The Evaluation of Variations in Patterns of Sphenoid Sinus Pneumatization Using Computed Tomography in a South Indian Population.Cureus. 2022 Mar 15;14(3):e23174. doi: 10.7759/cureus.23174. eCollection 2022 Mar. Cureus. 2022. PMID: 35433147 Free PMC article.
-
Carotid canal and optic canal at sphenoid sinus.Neurosurg Rev. 2019 Jun;42(2):519-529. doi: 10.1007/s10143-018-0995-4. Epub 2018 Jun 21. Neurosurg Rev. 2019. PMID: 29926302
References
-
- Cavallo L M, Messina A, Cappabianca P, et al. Endoscopic endonasal surgery of the midline skull base: anatomical study and clinical considerations. Neurosurg Focus. 2005;19:E2. - PubMed
-
- Hamberger C A, Hammer G, Norlen G. Transphenoidal hypophysectomy. Arch Otolaryngol. 1961;74:2–8. - PubMed
-
- Batra P S, Citardi M J, Gallivan R P, Roh H J, Lanza D C. Software-enabled computed tomography analysis of the carotid artery and sphenoid sinus pneumatization patterns. Am J Rhinol. 2004;18:203–208. - PubMed
-
- Scuderi A J, Harnsberger H R, Boyer R S. Pneumatization of the paranasal sinuses: normal features of importance to the accurate interpretation of CT scans and MR images. AJR Am J Roentgenol. 1993;160:1101–1104. - PubMed
-
- Romano A, Zuccarello M, Loveren H R Van, Keller J T. Expanding the boundaries of the trans-sphenoidal approach: a micro anatomic study. Clin Anat. 2001;14:1–9. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
