

doi: 10.1055/s-2007-994292.
Proposed classification for the transbasal approach and its modifications
Affiliations
- PMID: 18592024
- PMCID: PMC2435472
- DOI: 10.1055/s-2007-994292
Item in Clipboard
Proposed classification for the transbasal approach and its modifications
Skull Base.
2008 Jan.
Abstract
The transbasal approach offers extradural exposure of the anterior midline skull base transcranially. It can be used to treat a variety of conditions, including trauma, craniofacial deformity, and tumors. This approach has been modified to enhance basal access. This article reviews the principle differences among modifications to the transbasal approach and introduces a new classification scheme. The rationale is to offer a uniform nomenclature to facilitate discussion of these approaches, their indications, and related issues.
Keywords: Frontal fossa; skull base; subcranial; subfrontal; transbasal.
Figures
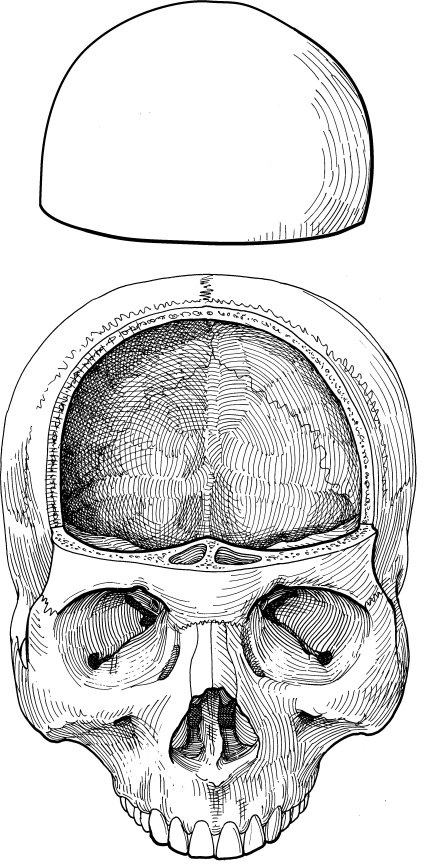
The transbasal approach consists of a frontal craniotomy without any osteotomies of the orbital bar or nasion. (Reprinted with permission from Barrow Neurological Institute, Phoenix, AZ.)
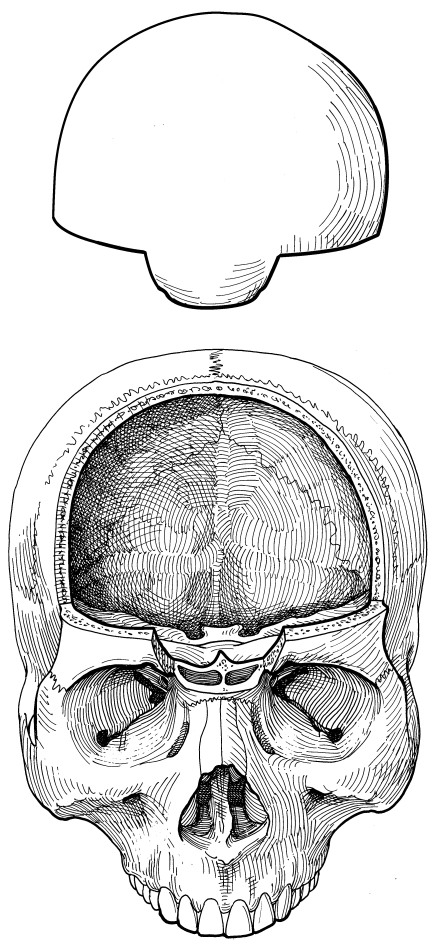
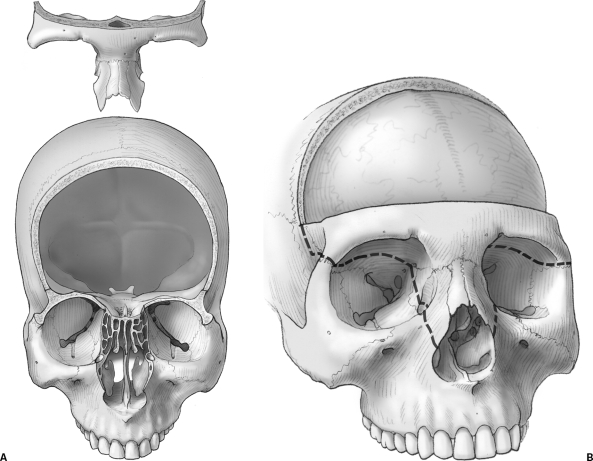
The level I transbasal approach adds any orbital bar osteotomy to a frontal craniotomy. The medial canthal ligaments are not violated. Here, the nasion is included in a one-piece fashion with the frontal craniotomy flap. (Reprinted with permission from Barrow Neurological Institute, Phoenix, AZ.)
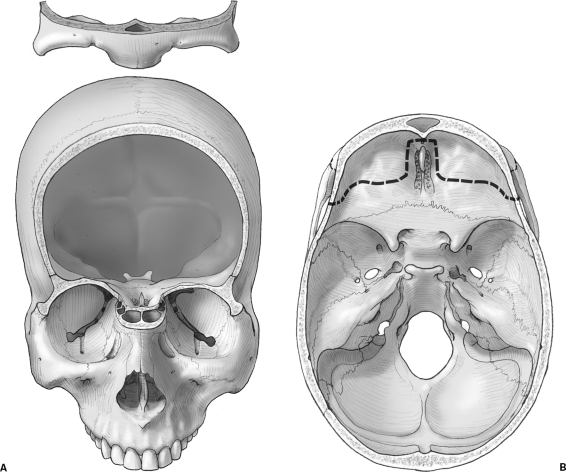
Here, the extent of orbital osteotomies for a level I transbasal approach varies depending on the surgical need. (A) The entire orbital rim and nasion are included. (B) The osteotomy line is indicated as a dashed line traversing the frontal fossa. (Reprinted from Lawton MT, Beals SP, Joganic EF, Han PP, Spetzler RF. The transfacial approaches to midline skull base lesions: a classification scheme. Operative Techniques in Neurosurgery 1999;2:1–18, with permission from Elsevier.)
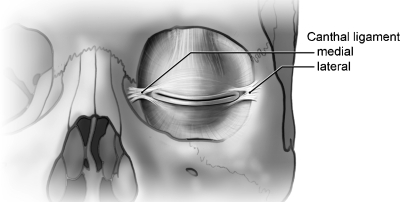
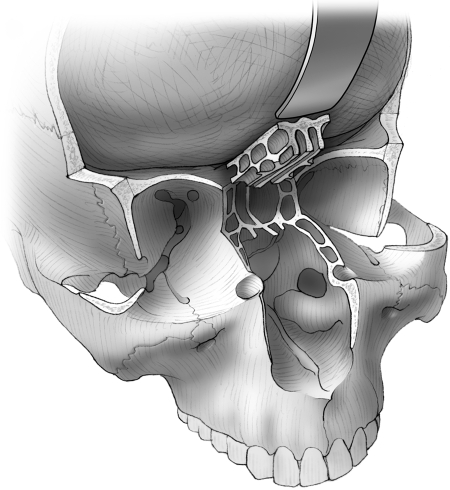
The anatomy of the canthal ligaments is outlined. The status of their integrity is a key component for classification of transbasal approaches. (Reprinted with permission from Barrow Neurological Institute, Phoenix, AZ.)
Here, the extent of naso-orbital osteotomies for a level II transbasal approach varies depending on the surgical need. (A) The entire orbital rim and nasal bone are included. (B) The osteotomy line is indicated as a dashed line traversing the frontal fossa and facial structures. (Reprinted from Lawton MT, Beals SP, Joganic EF, Han PP, Spetzler RF. The transfacial approaches to midline skull base lesions: a classification scheme. Operative Techniques in Neurosurgery 1999;2:1–18, with permission from Elsevier.)
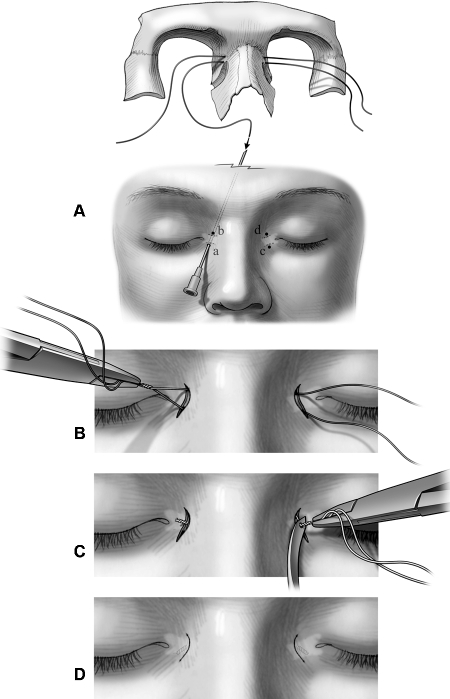
A medial canthopexy is required after a level II or III transbasal approach because, by definition, the medial canthal ligaments are taken down uni- or bilaterally. (A) Bilateral medial canthopexies are performed using two 28-gauge wires that are passed above and below the medial canthus through puncture holes (labeled as a, b, c, and d) created with an 18-gauge needle. (B) A clamp or needle holder is used to twist ipsilateral wires clockwise about four 360-degree turns. (C) The contralateral wires are then turned four 360-degree turns clockwise while they are placed under tension with a Tessier wire passer awl. (D) Finally, the twisted wire ends are trimmed and buried in the subcutaneous tissue around the medial canthus, and the small semilunar skin incisions are closed with fast-absorbing gut sutures. (Reprinted with permission from Feiz-Erfan I, Han PP, Spetzler RF, et al. The radical transbasal approach for resection of anterior and midline skull base lesions. J Neurosurg 2005;103:485–490.)
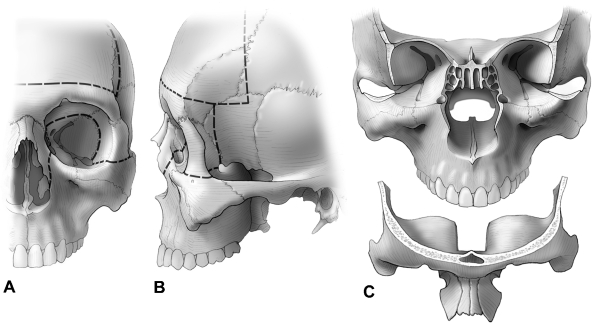
The (A) frontal and (B) lateral surface views of the skull indicate the osteotomy lines for a level III transbasal approach. (C) The extended orbital bar osteotomy is shown as resected in a bilateral osteotomy. Again, the extent of a level III transbasal approach can be tailored to the pathology. By definition, one medial and one lateral canthus on the same side are taken down with the osteotomy to incorporate at least one infraorbital fissure located on the side of medial canthus detachment. (Reprinted with permission from Feiz-Erfan I, Han PP, Spetzler RF, et al. The radical transbasal approach for resection of anterior and midline skull base lesions. J Neurosurg 2005;103:485–490.)
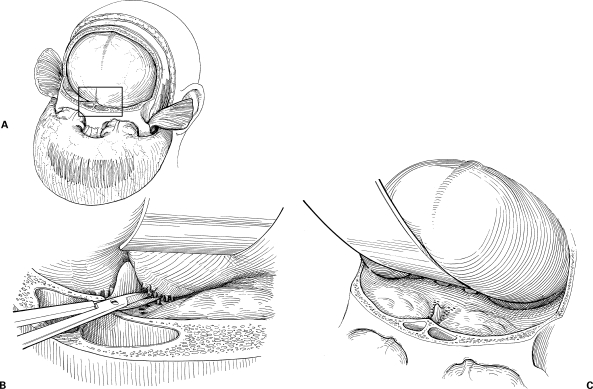
(A) Traditionally, the transbasal approach (inset, area of interest) requires (B) sacrifice of the olfactory fila. (C) This maneuver allows the frontal dura to be retracted and provides extradural access to the frontal skull base. (Reprinted with permission from Barrow Neurological Institute, Phoenix, AZ.)
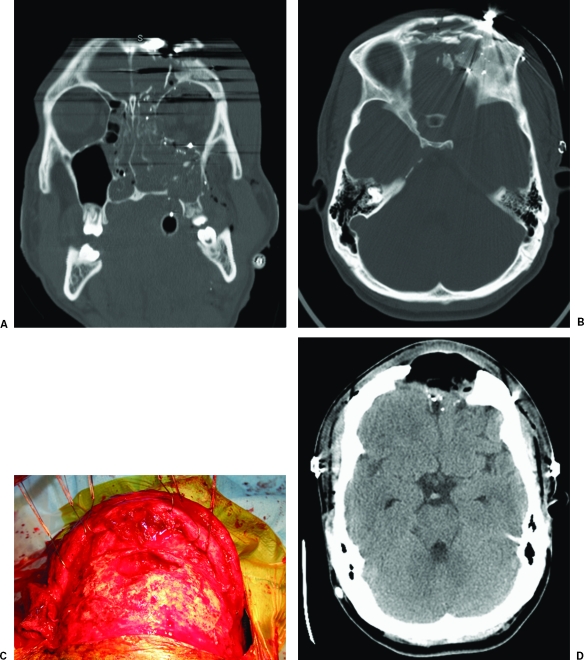
The transbasal approach is well suited for managing anterior skull base trauma. (A) Coronal and (B) axial bone window computed tomography (CT) scans of the head show multiple craniofacial and skull base fractures associated with an open scalp laceration after direct blunt injury. A transbasal approach was used to repair and close the cerebrospinal fluid leak. Due to the increased risk of infection, no orbital bar osteotomies were included. (C) Six months after surgery, the patient underwent surgical débridement of purulent infection with loss of the frontal bone flap, as seen during the procedure and on a (D) postoperative bone window CT of the head. The initial use of the transbasal approach prevented the functionally and cosmetically important orbital bar from being lost to infection.
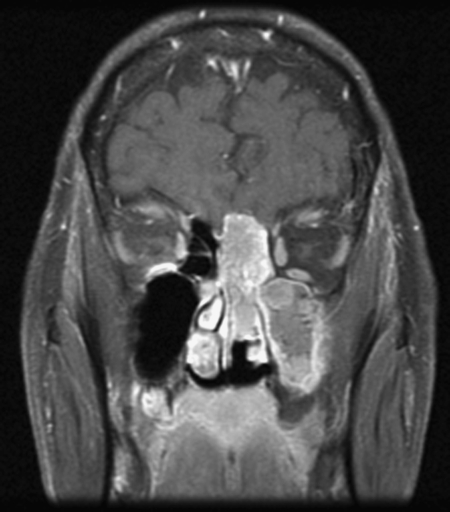
Contrasted T1-weighted magnetic resonance image shows an olfactory neuroblastoma, which was resected through a level I transbasal approach (bifrontal craniotomy with attached one-piece osteotomy of the nasion) combined with a transfacial approach.
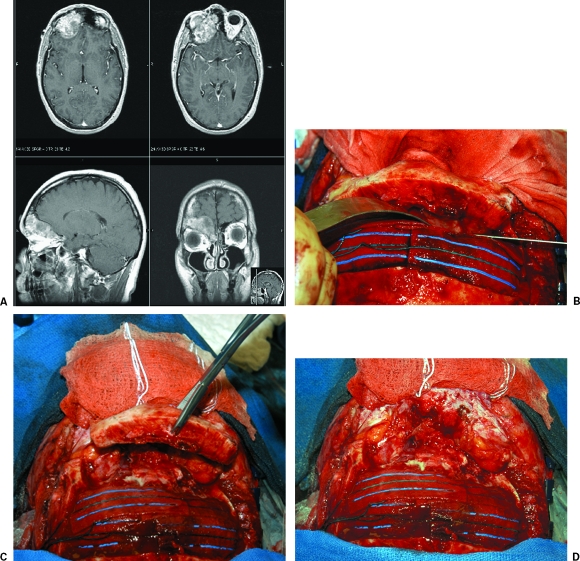
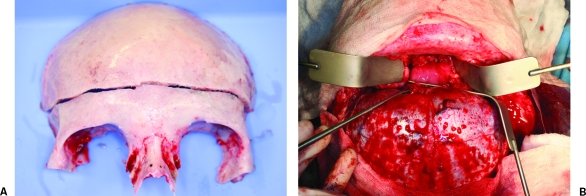
(A) Magnetic resonance images of the brain show fibrous dysplasia of the orbital bar. (B) Operative photographs show the thickened orbital bar, which has been (C) osteotomized without violation of the medial canthal ligaments (level I transbasal approach). (D) The intraorbital exposure after removal of the orbital bar.
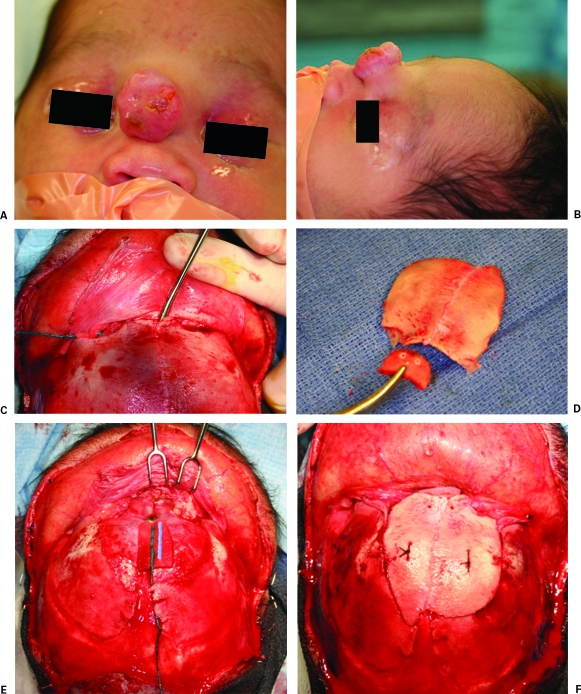
(A) Anterior and (B) lateral photographs of a baby with a frontal encephalocele. (C) The lesion is outlined with a dissector after a bicoronal scalp incision is performed. (D) The frontal craniotomy flap. A split calvarium graft is used to reconstruct the nasion (level I transbasal approach). (E) After the encephalocele is resected, the bony defect involving the nasion is visible. (F) The defect is reconstructed with the bony fragments seen in (D).
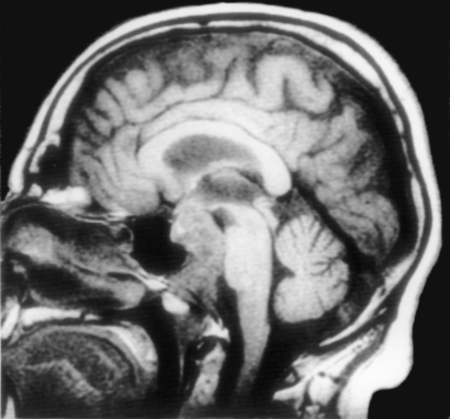
Sagittal T1-weighted magnetic resonance image shows a clival chordoma that was resected via a level II transbasal approach. (Reprinted with permission from Barrow Neurological Institute, Phoenix, AZ.)
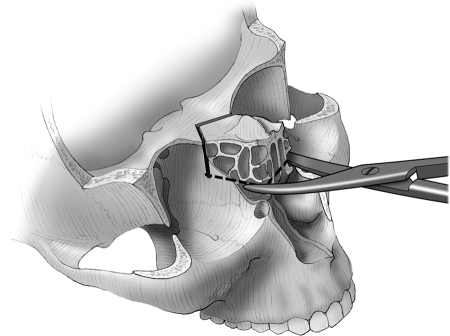
The nasal mucosal cuff is cut with heavy, curved scissors 1 to 2 cm below the cribriform plate in an attempt to preserve olfaction during a cribriform plate osteotomy (dashed line). (Reprinted with permission from Barrow Neurological Institute, Phoenix, AZ.)
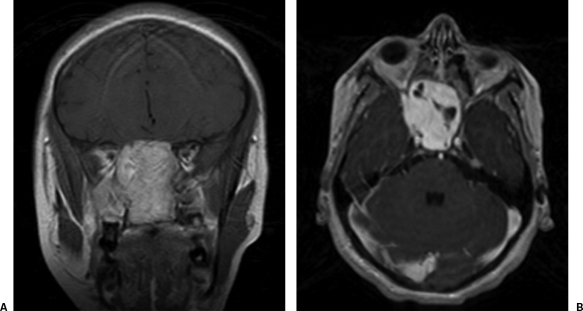
Contrasted (A) coronal and (B) axial magnetic resonance images show a large juvenile angiofibroma.
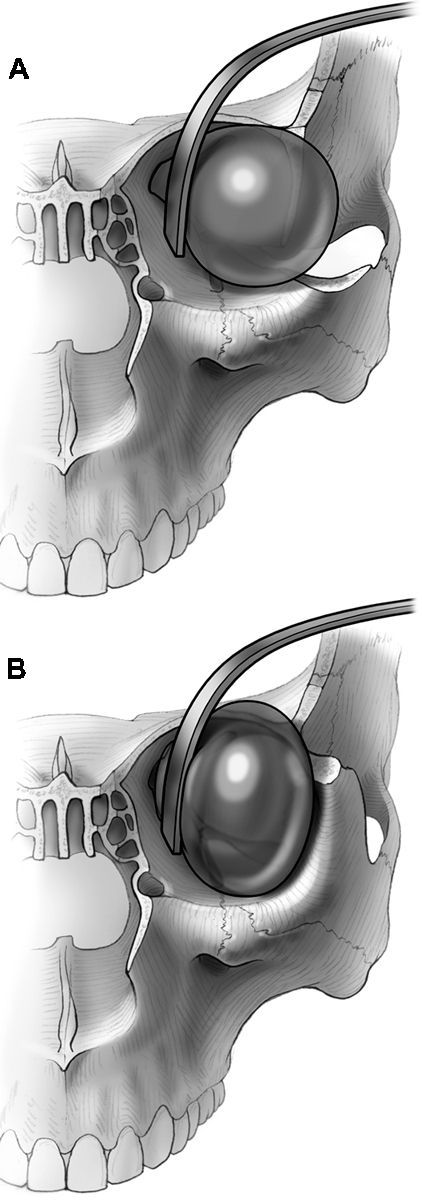
(A) Osteotomizing the lateral orbital wall down to the infraorbital fissure minimizes retraction pressure on the orbital contents, (B) compared with leaving the lateral orbital wall in place. (Reprinted with permission from Feiz-Erfan I, Han PP, Spetzler RF, et al. The radical transbasal approach for resection of anterior and midline skull base lesions. J Neurosurg 2005;103:485–490.)
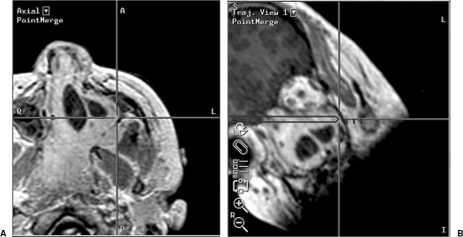
(A) Axial localizing and (B) trajectory neuronavigational views show the microscopic point of focus to be located on the lateral wall of the maxillary sinus. This microscopic view was achieved during craniofacial surgery for resection of a large juvenile angiofibroma via a level III transbasal approach.
After the cribriform plate osteotomy is completed, the cribriform plate and frontal dura are retracted to allow basal access. (Reprinted with permission from Barrow Neurological Institute, Phoenix, AZ.)
(A) After a level III transbasal approach is performed and (B) the juvenile angiofibroma is exposed transcranially, the cribriform plate is retracted along with the frontal dura (a surgical dissector points to the cribriform plate). Lateral retraction of the contents of both orbits maximizes the corridor into the sinonasal cavity. Bilateral osteotomies of the lateral orbital walls minimize retraction pressure on the orbital contents.
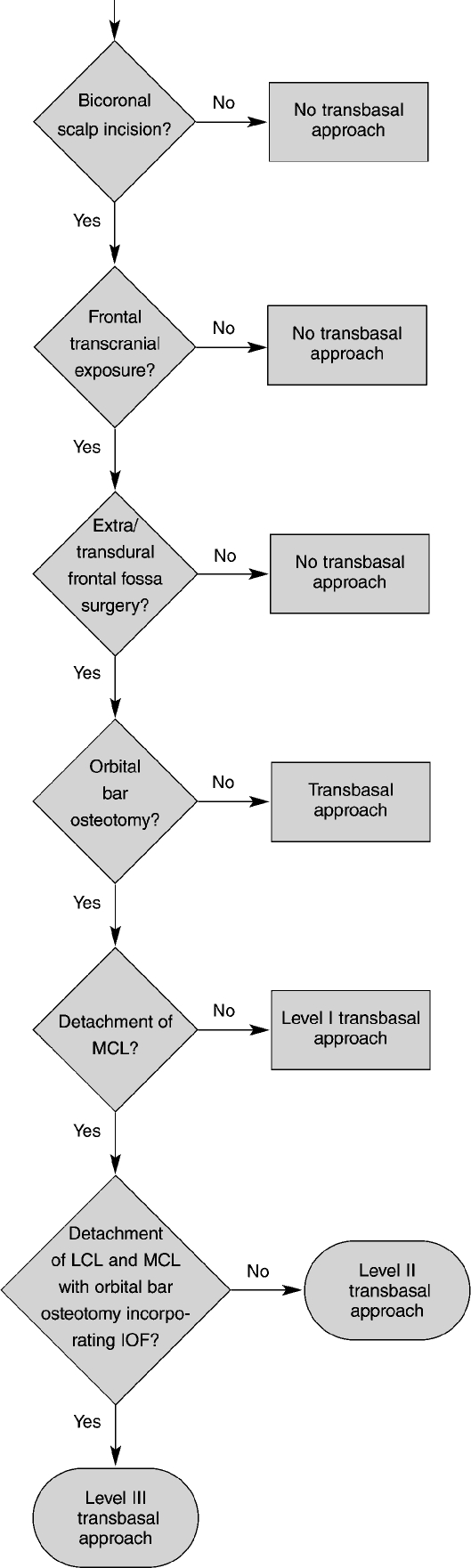
A decision tree outlines key differences and similarities among the transbasal approaches. MCL, medial canthal ligament; LCL, lateral canthal ligament; IOF, inferior orbital fissure. (Reprinted with permission from Barrow Neurological Institute, Phoenix, AZ.)
Similar articles
-
Anatomical Step-by-Step Dissection of Complex Skull Base Approaches for Trainees: Surgical Anatomy of the Bifrontal Transbasal Approach, Surgical Principles, and Illustrative Cases.J Neurol Surg B Skull Base. 2023 Oct 9;85(6):596-605. doi: 10.1055/s-0043-1775875. eCollection 2024 Dec. J Neurol Surg B Skull Base. 2023. PMID: 39483163 Free PMC article.
-
The radical transbasal approach for resection of anterior and midline skull base lesions.J Neurosurg. 2005 Sep;103(3):485-90. doi: 10.3171/jns.2005.103.3.0485. J Neurosurg. 2005. PMID: 16235681
-
The extended transbasal approach: a quantitative anatomical and histological study.Acta Neurochir (Wien). 1999;141(3):251-9. doi: 10.1007/s007010050295. Acta Neurochir (Wien). 1999. PMID: 10214481
-
Extended transbasal approach to skull base tumors. Technical nuances and review of the literature.Oncology (Williston Park). 2005 Jun;19(7):913-9; discussion 920, 923-5, 929. Oncology (Williston Park). 2005. PMID: 16053038 Review.
-
Combined Endoscopic and Open Approaches in the Management of Sinonasal and Ventral Skull Base Malignancies.Otolaryngol Clin North Am. 2017 Apr;50(2):331-346. doi: 10.1016/j.otc.2016.12.009. Otolaryngol Clin North Am. 2017. PMID: 28314401 Review.
Cited by
-
The interhemispheric fissure-surgical outcome of interhemispheric approaches.Neurosurg Rev. 2021 Aug;44(4):2099-2110. doi: 10.1007/s10143-020-01372-6. Epub 2020 Aug 27. Neurosurg Rev. 2021. PMID: 32852637 Free PMC article.
-
Combined craniofacial resection of anterior skull base tumors: long-term results and experience of single institution.Neurosurg Rev. 2011 Jan;34(1):101-13. doi: 10.1007/s10143-010-0286-1. Epub 2010 Sep 29. Neurosurg Rev. 2011. PMID: 20878534
-
Midline Meningiomas of the Anterior Skull Base: Surgical Outcomes and a Decision-Making Algorithm for Classic Skull Base Approaches.Cancers (Basel). 2020 Nov 3;12(11):3243. doi: 10.3390/cancers12113243. Cancers (Basel). 2020. PMID: 33153110 Free PMC article.
-
The transbasal approach to the anterior skull base: surgical outcome of a single-centre case series.Sci Rep. 2020 Dec 31;10(1):22444. doi: 10.1038/s41598-020-80255-8. Sci Rep. 2020. PMID: 33384441 Free PMC article.
-
Clinicopathological features of cranial-nasal-orbital communicating lesions and diagnostic indicators for differentiating benign and malignant neoplasms.Int J Ophthalmol. 2025 Jul 18;18(7):1357-1368. doi: 10.18240/ijo.2025.07.20. eCollection 2025. Int J Ophthalmol. 2025. PMID: 40688786 Free PMC article.
References
-
- Beals S P, Joganic E. Transfacial exposure of anterior cranial fossa and clival tumors. BNI Q. 1992;8:2–18.
-
- Raso J L, Gusmäo S. Transbasal approach to skull base tumors: evaluation and proposal of classification. Surg Neurol. 2006;65(suppl 1):S1:33–S1:37. discussion 1:37–1:38. - PubMed
-
- Dandy W E. Orbital Tumors: Results Following the Transcranial Operative Attack. New York: Oskar Piest; 1941.
-
- Unterberger S. Care of frontobasal wounds [in German] Arch Ohren Nasen Kehlkopfheilkd. 1958;172:463–484. - PubMed
-
- Tessier P, Guiot G, Derome P. Orbital hypertelorism: II. Definite treatment of orbital hypertelorism (OR.H.) by craniofacial or by extracranial osteotomies. Scand J Plast Reconstr Surg. 1973;7:39–58. - PubMed
