

Impact of hospital volume on the economic value of computer navigation for total knee replacement
- PMID: 18594098
- PMCID: PMC2657305
- DOI: 10.2106/JBJS.G.00888
Impact of hospital volume on the economic value of computer navigation for total knee replacement
Abstract
Background: An aim of the use of computer navigation is to reduce rates of revisions of total knee replacements by improving the alignment achieved at the surgery. However, the decision to adopt this technology may be difficult for some centers, especially low-volume centers, where the cost of purchasing this equipment may be high. The purpose of this study was to examine the impact of hospital volume on the cost-effectiveness of this new technology in order to determine its feasibility and the level of evidence that should be sought prior to its adoption.
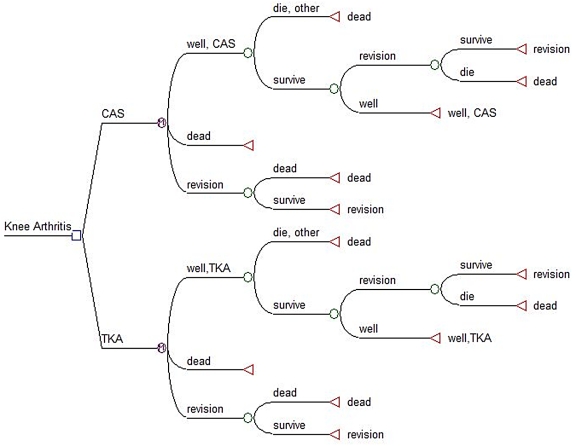
Methods: A Markov decision model was used to evaluate the impact of hospital volume on the cost-effectiveness of computer-assisted knee arthroplasty in a theoretical cohort of sixty-five-year-old patients with end-stage arthritis of the knee to coincide with the peak incidence of knee arthroplasty in the United States.
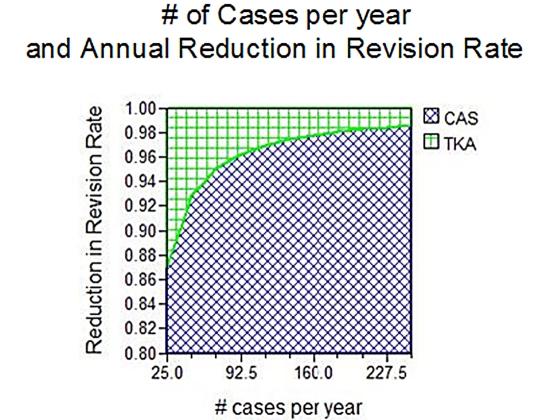
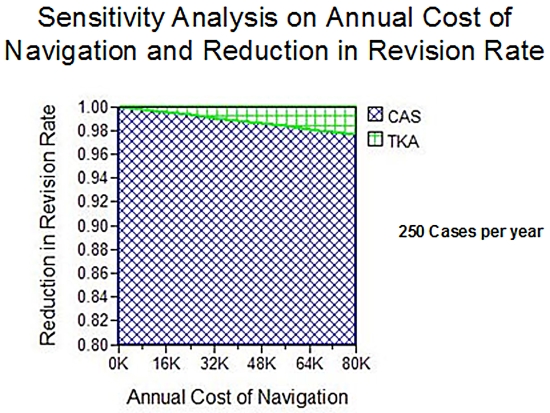
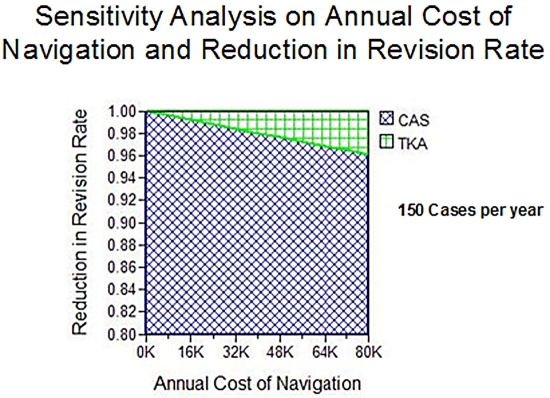
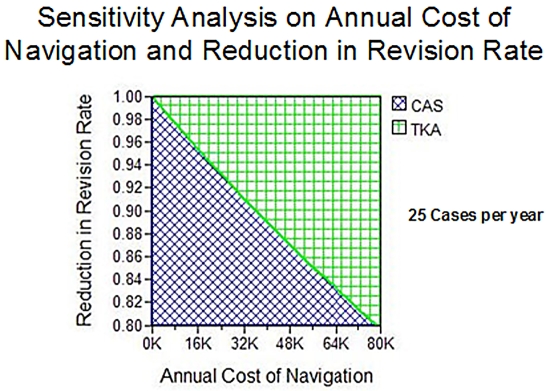
Results: Computer-assisted surgery becomes less cost-effective as the annual hospital volume decreases, as the cost of the navigation increases, and as the impact on revision rates decreases. Centers at which 250, 150, and twenty-five computer-navigated total knee arthroplasties are performed per year will require a reduction of the annual revision rate of 2%, 2.5%, and 13%, respectively, per year over a twenty-year period for computer navigation to be cost-effective.
Conclusions: Computer navigation is less likely to be a cost-effective investment in health-care improvement in centers with a low volume of joint replacements, where its benefit is most likely to be realized. However, it may be a cost-effective technology for centers with a higher volume of joint replacements, where the decrease in the rate of knee revision needed to make the investment cost-effective is modest, if improvements in revision rates with the use of this technology can be realized.
Figures
Similar articles
-
An economic model to evaluate cost-effectiveness of computer assisted knee replacement surgery in Norway.BMC Musculoskelet Disord. 2013 Jul 6;14:202. doi: 10.1186/1471-2474-14-202. BMC Musculoskelet Disord. 2013. PMID: 23829478 Free PMC article.
-
The cost-effectiveness of computer-assisted navigation in total knee arthroplasty.J Bone Joint Surg Am. 2007 Nov;89(11):2389-97. doi: 10.2106/JBJS.F.01109. J Bone Joint Surg Am. 2007. PMID: 17974880
-
Computer-assisted navigation in knee arthroplasty: a critical appraisal.J Knee Surg. 2013 Oct;26(5):357-61. doi: 10.1055/s-0033-1341581. Epub 2013 Mar 19. J Knee Surg. 2013. PMID: 23512544 Review.
-
Can Robot-Assisted Unicompartmental Knee Arthroplasty Be Cost-Effective? A Markov Decision Analysis.J Arthroplasty. 2016 Apr;31(4):759-65. doi: 10.1016/j.arth.2015.10.018. Epub 2015 Oct 26. J Arthroplasty. 2016. PMID: 26706836
-
Technology and cost-effectiveness in knee arthroplasty: computer navigation and robotics.Am J Orthop (Belle Mead NJ). 2009 Feb;38(2 Suppl):32-6. Am J Orthop (Belle Mead NJ). 2009. PMID: 19340382 Review.
Cited by
-
The cost-effectiveness of surgical treatment of medial unicompartmental knee osteoarthritis in younger patients: a computer model-based evaluation.J Bone Joint Surg Am. 2015 May 20;97(10):807-17. doi: 10.2106/JBJS.N.00925. J Bone Joint Surg Am. 2015. PMID: 25995491 Free PMC article.
-
Volume-outcome relationships in laryngeal trauma processes of care: a retrospective cohort study.Eur J Trauma Emerg Surg. 2022 Oct;48(5):4131-4141. doi: 10.1007/s00068-022-01950-x. Epub 2022 Mar 23. Eur J Trauma Emerg Surg. 2022. PMID: 35320370
-
The cost-effectiveness of computer navigation in primary total knee replacement: a scoping review.EFORT Open Rev. 2021 Mar 1;6(3):173-180. doi: 10.1302/2058-5241.6.200073. eCollection 2021 Mar. EFORT Open Rev. 2021. PMID: 33841916 Free PMC article.
-
Assessing the value of a total joint replacement.Curr Rev Musculoskelet Med. 2012 Dec;5(4):274-82. doi: 10.1007/s12178-012-9139-6. Curr Rev Musculoskelet Med. 2012. PMID: 23054621 Free PMC article.
-
Augmented reality-based navigation system applied to tibial bone resection in total knee arthroplasty.J Exp Orthop. 2019 Nov 11;6(1):44. doi: 10.1186/s40634-019-0212-6. J Exp Orthop. 2019. PMID: 31712907 Free PMC article.
References
-
- Mahomed NN, Barrett JA, Katz JN, Phillips CB, Losina E, Lew RA, Guadagnoli E, Harris WH, Poss R, Baron JA. Rates and outcomes of primary and revision total hip replacement in the United States Medicare population. J Bone Joint Surg Am. 2003;85:27-32. - PubMed
-
- Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89:780-5. - PubMed
-
- Katz JN, Barrett J, Mahomed NN, Baron JA, Wright RJ, Losina E. Association between hospital and surgeon procedure volume and the outcomes of total knee replacement. J Bone Joint Surg Am. 2004;86:1909-16. - PubMed
-
- Soohoo NF, Zingmond DS, Lieberman JR, Ko CY. Primary total knee arthroplasty in California 1991 to 2001: does hospital volume affect outcomes? J Arthroplasty. 2006;21:199-205. - PubMed
-
- Bozic KJ, Katz P, Cisternas M, Ono L, Ries MD, Showstack J. Hospital resource utilization for primary and revision total hip arthroplasty. J Bone Joint Surg Am. 2005;87:570-6. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
