

Alternative approaches to endoscopic ablation for benign enlargement of the prostate: systematic review of randomised controlled trials
- PMID: 18595932
- PMCID: PMC2443595
- DOI: 10.1136/bmj.39575.517674.BE
Alternative approaches to endoscopic ablation for benign enlargement of the prostate: systematic review of randomised controlled trials
Abstract
Objective: To compare the effectiveness and risk profile of newer methods for endoscopic ablation of the prostate against the current standard of transurethral resection.
Design: Systematic review and meta-analysis.
Data sources: Electronic and paper records in subject area up to March 2006.
Review methods: We searched for randomised controlled trials of endoscopic ablative interventions that included transurethral resection of prostate as one of the treatment arms. Two reviewers independently extracted data and assessed quality. Meta-analyses of prespecified outcomes were done using fixed and random effects models and reported using relative risk or weighted mean difference.
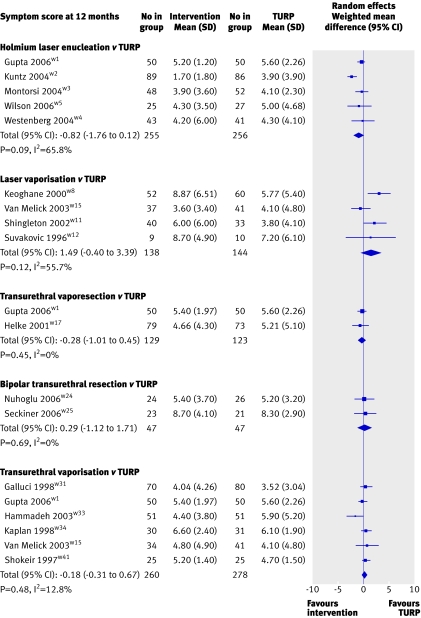
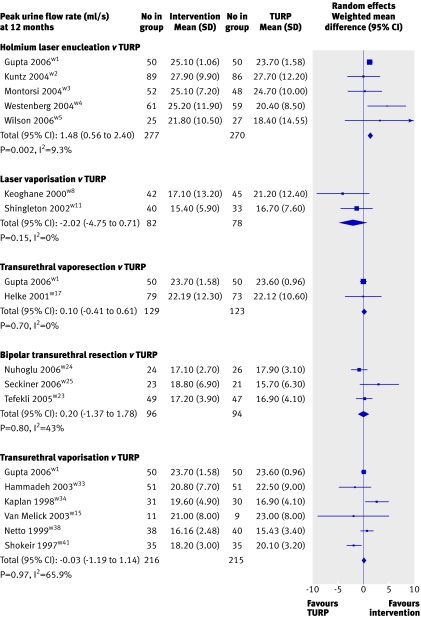
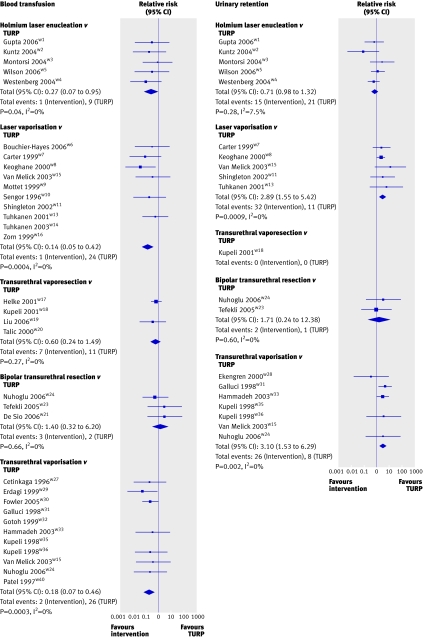
Results: We identified 45 randomised controlled trials meeting the inclusion criteria and reporting on 3970 participants. The reports were of moderate to poor quality, with small sample sizes. None of the newer technologies resulted in significantly greater improvement in symptoms than transurethral resection at 12 months, although a trend suggested a better outcome with holmium laser enucleation (random effects weighted mean difference -0.82, 95% confidence interval 1.76 to 0.12) and worse outcome with laser vaporisation (1.49, -0.40 to 3.39). Improvements in secondary measures, such as peak urine flow rate, were consistent with change in symptoms. Blood transfusion rates were higher for transurethral resection than for the newer methods (4.8% v 0.7%) and men undergoing laser vaporisation or diathermy vaporisation were more likely to experience urinary retention (6.7% v 2.3% and 3.6% v 1.1%). Hospital stay was up to one day shorter for the newer technologies.
Conclusions: Although men undergoing more modern methods of removing benign prostatic enlargement have similar outcomes to standard transurethral resection of prostate along with fewer requirements for blood transfusion and shorter hospital stay, the quality of current evidence is poor. The lack of any clearly more effective procedure suggests that transurethral resection should remain the standard approach.
Conflict of interest statement
Competing interests: None declared.
Figures
Comment in
-
Endoscopic ablation for benign enlargement of the prostate.BMJ. 2008 Jun 30;337(7660):a535. doi: 10.1136/bmj.39582.425417.BE. BMJ. 2008. PMID: 18595937 Free PMC article.
-
Endoscopic ablation: Irreversible tide of technological advancement?BMJ. 2008 Jul 22;337:a903. doi: 10.1136/bmj.a903. BMJ. 2008. PMID: 18647782 No abstract available.
References
-
- Emberton M, Neal DE, Black N, Harrison M, Fordham M, McBrien MP, et al. The national prostatectomy audit: the clinical management of patients during hospital admission. Br J Urol 1995;75:301-16. - PubMed
-
- Mebust WK, Holtgrewe HL, Cockett AT, Peters PC. Transurethral prostatectomy: immediate and postoperative complications. A cooperative study of 13 participating institutions evaluating 3,885 patients. J Urol 1989;141:243-7. - PubMed
-
- Undertaking systematic reviews of research on effectiveness. CRD’s guidance for those carrying out or commissioning reviews. CRD report No 4 University of York: Centre for Reviews and Dissemination, 2001
-
- Verhagen AP, de Vet HC, de Bie RA, Kessels AG, Boers M, Bouter LM, et al. The Delphi list: a criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi consensus. J Clin Epidemiol 1998;51:1235-41. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical