

Is office-based counseling about media use, timeouts, and firearm storage effective? Results from a cluster-randomized, controlled trial
- PMID: 18595960
- PMCID: PMC4486046
- DOI: 10.1542/peds.2007-2611
Is office-based counseling about media use, timeouts, and firearm storage effective? Results from a cluster-randomized, controlled trial
Abstract
Objective: The objective of this study was to determine whether patients' families' violence-prevention behaviors would be affected by their primary care practitioner's use of a violence-prevention clinical intervention during the routine well-child examination.
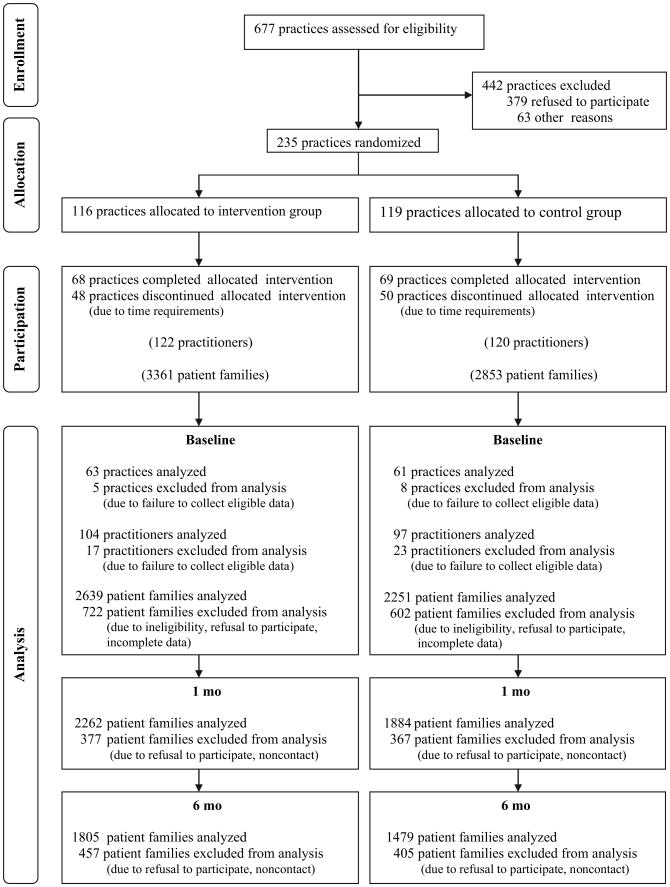
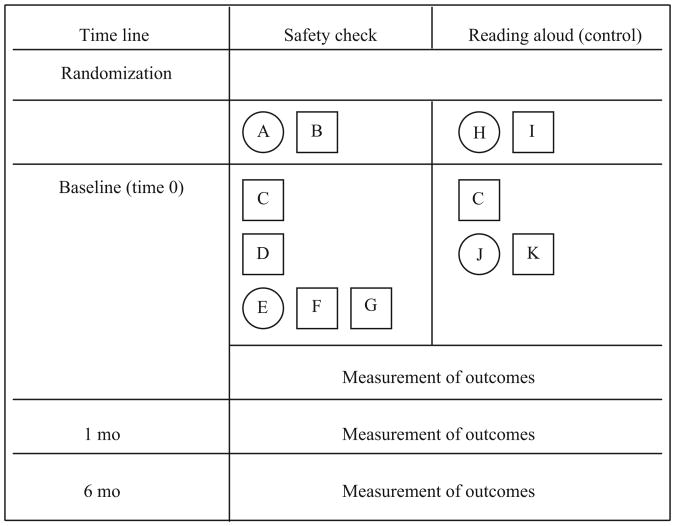
Methods: In this cluster-randomized, controlled trial (2002-2006), 137 Pediatric Research in Office Settings practices were randomly assigned and initiated patient recruitment for either an office-based violence-prevention intervention or a control group (educational handout on literacy promotion provided). Primary caregivers of children who were aged 2 to 11 years and presented for a well-child visit were surveyed at baseline and 1 and 6 months. Practitioners were trained to (1) review a parent previsit summary regarding patient-family behavior and parental concern about media use, discipline strategies, and children's exposure to firearms, (2) counsel using brief principles of motivational interviewing, (3) identify and provide local agency resources for anger and behavior management when indicated, and (4) instruct patient-families on use of tangible tools (minute timers to monitor media time/timeouts and firearm cable locks to store firearms more safely where children live or play). Main outcomes were change over time in self-reported media use <120 minutes per day, use of timeouts, and use of firearm cable locks.
Results: Generalized estimating equation analysis revealed a significant effect at 6 months for decreased media use and safer firearm storage. The intervention group compared with the control group showed an increase in limiting media use to <120 minutes per day. There was no significant effect for timeout use. There was a substantial increase in storing firearms with cable locks for the intervention group versus a decrease for the control group.
Conclusions: This randomized, controlled trial demonstrated decreased media exposure and increased safe firearm storage as a result of a brief office-based violence-prevention approach.
Figures
References
-
- Cook P, Ludwig J. Aiming for evidence-based gun policy. J Policy Anal Manage. 2006;25(3):691–735.
-
- Centers for Disease Control and Prevention. Deaths: Preliminary Data for 2004. [Accessed January 25, 2007];Natl Vital Stat Rep. 2006 45(19) Available at: www.cdc.gov/nchs/data/nvsr/nvsr54/nvsr54_19.pdf. - PubMed
-
- DuRant RH, Treiber F, Goodman E, Woods ER. Intentions to use violence among young adolescents. Pediatrics. 1996;98(6 pt 1):1104–1108. - PubMed
-
- DuRant RH, Champion H, Wolfson M. The relationship between watching professional wrestling on television and engaging in date fighting among high school students. Pediatrics. 2006;118(2) Available at: www.pediatrics.org/cgi/content/full/118/2/e265. - PubMed
