

Pediatric traumatic brain injury is inconsistently regionalized in the United States
- PMID: 18595962
- PMCID: PMC2562242
- DOI: 10.1542/peds.2007-3399
Pediatric traumatic brain injury is inconsistently regionalized in the United States
Abstract
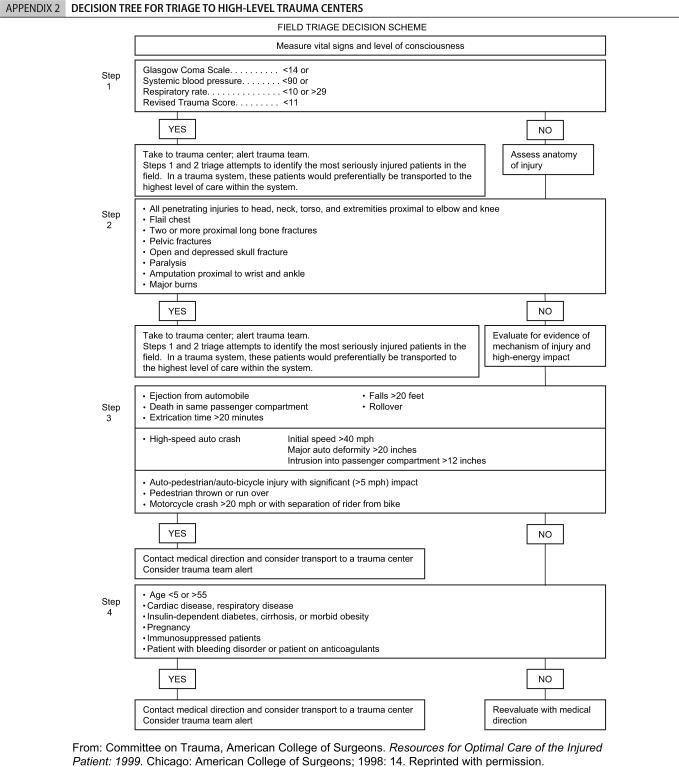
Objectives: Traumatic brain injury is a leading cause of death in children. On the basis of evidence of better outcomes, the American College of Surgery Committee on Trauma recommends that children with severe traumatic brain injury receive care at high-level trauma centers. We assessed rates of adherence to these recommendations and factors associated with adherence.
Methods: We studied population and hospital discharge data from 2001 from all of the health care referral regions (n = 68) in 6 US states (Florida, Massachusetts, New Jersey, New York, Texas, and Virginia). We identified children with severe traumatic brain injury by using International Classification of Diseases, Ninth Revision, Clinical Modification, codes and American College of Surgery Committee on Trauma criteria. We defined "high-level centers" as either level I or pediatric trauma centers. We considered an area to be well regionalized if >or=90% of severe traumatic brain injury hospitalizations were in high-level centers. We also explored how use of level II trauma centers affected rates of care at high-level centers.
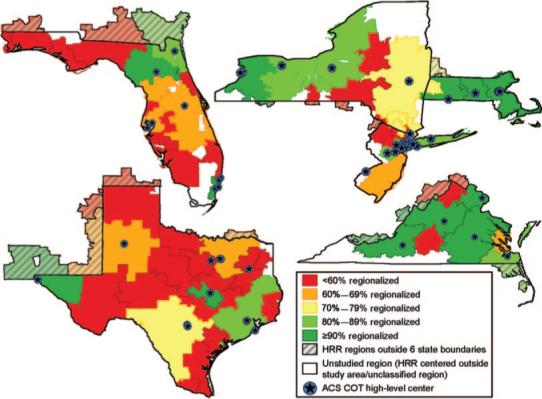
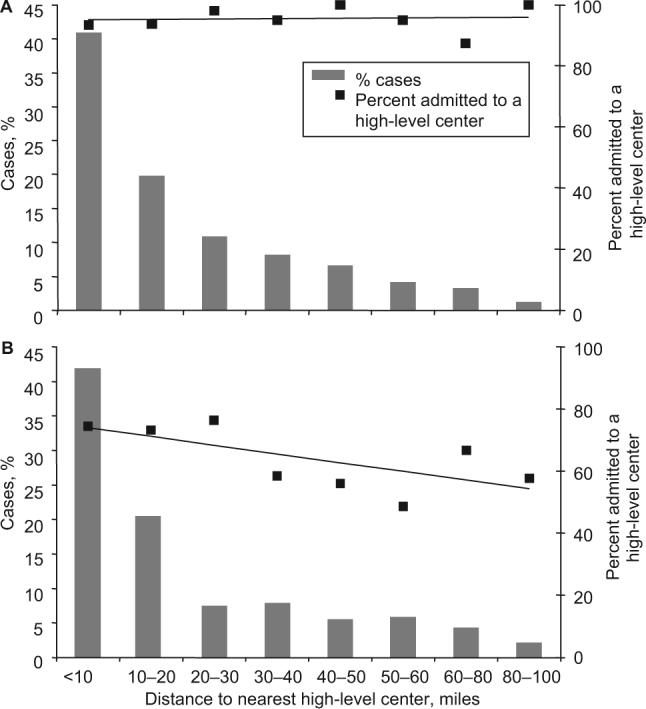
Results: Of 2117 admissions for severe pediatric traumatic brain injury, 67.3% were in high-level centers, and 87.3% were in either high-level or level II centers. Among states, 56.4% to 93.6% of severe traumatic brain injury admissions were in high-level centers. Only 2 states, Massachusetts and Virginia, were well regionalized. Across health care referral regions, 0% to 100% of severe traumatic brain injury admissions were in high-level centers, and only 19.1% of health care referral regions were well regionalized. Only a weak relationship existed between the distance to the nearest high-level center and regionalization. The age of statewide trauma systems had no relationship to the extent of regionalization.
Conclusions: Despite evidence for improved outcomes of severely injured children admitted to high-level trauma centers, we found that almost one third of the children with severe traumatic brain injury failed to receive care in such centers. Only 2 of 6 states and less than one fifth of 68 health care referral regions were well regionalized. This study highlights problems with current pediatric trauma care that can serve as a basis for additional research and health care policy.
Figures
Similar articles
-
Characteristics of pediatric trauma transfers to a level i trauma center: implications for developing a regionalized pediatric trauma system in california.Acad Emerg Med. 2010 Dec;17(12):1364-73. doi: 10.1111/j.1553-2712.2010.00926.x. Acad Emerg Med. 2010. PMID: 21122022 Free PMC article.
-
Patients with severe traumatic brain injury transferred to a Level I or II trauma center: United States, 2007 to 2009.J Trauma Acute Care Surg. 2012 Dec;73(6):1491-9. doi: 10.1097/TA.0b013e3182782675. J Trauma Acute Care Surg. 2012. PMID: 23188242
-
The effects of trauma center care, admission volume, and surgical volume on paralysis after traumatic spinal cord injury.Ann Surg. 2009 Jan;249(1):10-7. doi: 10.1097/SLA.0b013e31818a1505. Ann Surg. 2009. PMID: 19106669 Free PMC article.
-
The Epidemiology of Emergency Department Trauma Discharges in the United States.Acad Emerg Med. 2017 Oct;24(10):1244-1256. doi: 10.1111/acem.13223. Epub 2017 Sep 27. Acad Emerg Med. 2017. PMID: 28493608 Free PMC article.
-
Management of Spasticity After Traumatic Brain Injury in Children.Front Neurol. 2020 Feb 21;11:126. doi: 10.3389/fneur.2020.00126. eCollection 2020. Front Neurol. 2020. PMID: 32153498 Free PMC article. Review.
Cited by
-
Intensive care for pediatric traumatic brain injury.Intensive Care Med. 2013 Jan;39(1):129-36. doi: 10.1007/s00134-012-2748-0. Epub 2012 Nov 21. Intensive Care Med. 2013. PMID: 23179331
-
Neonatal and pediatric regionalized systems in pediatric emergency mass critical care.Pediatr Crit Care Med. 2011 Nov;12(6 Suppl):S128-34. doi: 10.1097/PCC.0b013e318234a723. Pediatr Crit Care Med. 2011. PMID: 22067921 Free PMC article.
-
Electronic clinical decision support for children with minor head trauma and intracranial injuries: a sociotechnical analysis.BMC Med Inform Decis Mak. 2021 May 19;21(1):161. doi: 10.1186/s12911-021-01522-w. BMC Med Inform Decis Mak. 2021. PMID: 34011315 Free PMC article.
-
Association between pediatric TBI mortality and median family income in the United States: A retrospective cohort study.Lancet Reg Health Am. 2022 Jan;5:100164. doi: 10.1016/j.lana.2021.100164. Epub 2022 Jan 5. Lancet Reg Health Am. 2022. PMID: 35252952 Free PMC article.
-
Facility characteristics and inhospital pediatric mortality after severe traumatic brain injury.J Neurotrauma. 2015 Jun 1;32(11):841-6. doi: 10.1089/neu.2014.3733. Epub 2015 May 8. J Neurotrauma. 2015. PMID: 25654233 Free PMC article.
References
-
- Langlois JA, Rutland-Brown W, Thomas KE. Traumatic Brain Injury in the United States: Emergency Department Visits, Hospitalizations, and Deaths. Centers for Disease Control; Atlanta, GA: 2004.
-
- Nathens AB, Jurkovich GJ, Maier RV, et al. Relationship between trauma center volume and outcomes. JAMA. 2001;285(9):1164–1171. - PubMed
-
- Mullins RJ, Mann NC, Hedges JR, Worrall W, Jurkovich GJ. Preferential benefit of implementation of a statewide trauma system in one of two adjacent states. J Trauma. 1998;44(4):609–616. - PubMed
-
- Nathens AB, Jurkovich GJ, Rivara FP, Maier RV. Effectiveness of state trauma systems in reducing injury-related mortality: a national evaluation. J Trauma. 2000;48(1):25–30. - PubMed
-
- Dudley RA, Johansen KL, Brand R, Rennie DJ, Milstein A. Selective referral to high-volume hospitals: estimating potentially avoidable deaths. JAMA. 2000;283(9):1159–1166. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
