

Patient factors used by pediatricians to assign asthma treatment
- PMID: 18595964
- PMCID: PMC2725186
- DOI: 10.1542/peds.2007-2271
Patient factors used by pediatricians to assign asthma treatment
Abstract
Objective: Although asthma is often inappropriately treated in children, little is known about what information pediatricians use to adjust asthma therapy. The purpose of this work was to assess the importance of various dimensions of patient asthma status as the basis of pediatrician treatment decisions.
Patients and methods: We conducted a cross-sectional, random-sample survey, between November 2005 and May 2006, of 500 members of the American Academy of Pediatrics using standardized case vignettes. Vignettes varied in regard to (1) acute health care use (hospitalized 6 months ago), (2) bother (parent bothered by the child's asthma status), (3) control (frequency of symptoms and albuterol use), (4) direction (qualitative change in symptoms), and (5) wheezing during physical examination. Our primary outcome was the proportion of pediatricians who would adjust treatment in the presence or absence of these 5 factors.
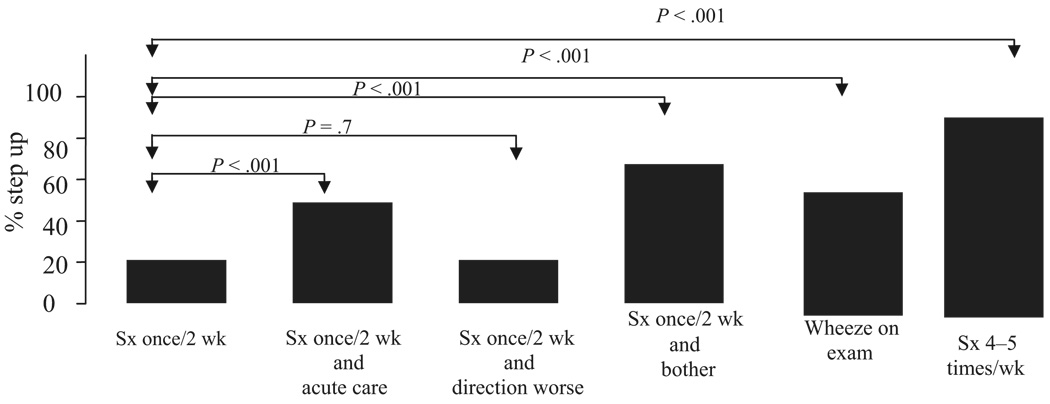
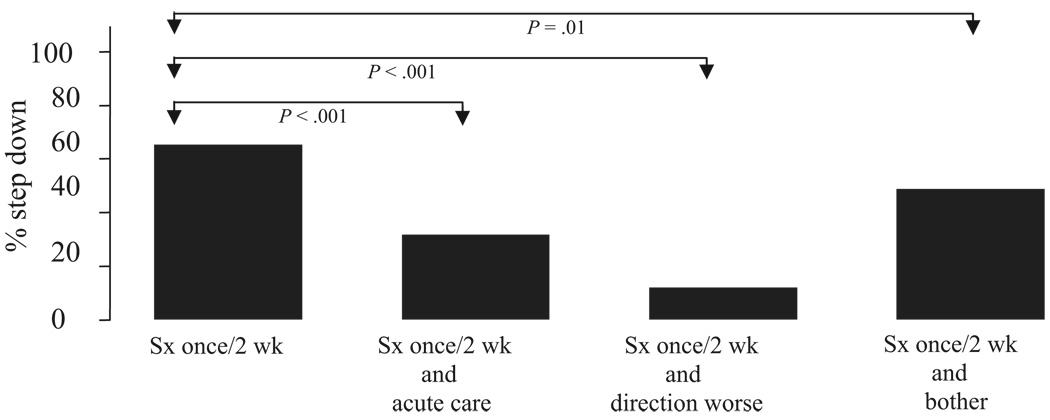
Results: Physicians used multiple dimensions of asthma status other than symptoms to determine treatment. Pediatricians were significantly more likely to increase treatment for a recently hospitalized patient (45% vs 18%), a bothered parent (67% vs 18%), poorly controlled symptoms (4-5 times per week; 100% vs 18%), or if there was wheezing on examination (45% vs 18%) compared with patients who only had well-controlled symptoms. Pediatricians were significantly less likely to decrease treatment for a child with well-controlled symptoms and recent hospitalization (28%), parents who reported being bothered (43%), or a child whose symptoms had worsened since the last doctor visit (10%) compared with children with well-controlled symptoms alone.
Conclusions: Pediatricians treat asthma on the basis of multiple dimensions of asthma status, including hospitalization, bother, symptom frequency, direction, and wheezing but use these factors differently to increase and decrease treatment. Tools that systematically assess multiple dimensions of asthma may be useful to help further improve pediatric asthma care.
Figures
Similar articles
-
Patient factors that physicians use to assign asthma treatment.Arch Intern Med. 2007 Jul 9;167(13):1360-6. doi: 10.1001/archinte.167.13.1360. Arch Intern Med. 2007. PMID: 17620528
-
Racial/ethnic variation in parent expectations for antibiotics: implications for public health campaigns.Pediatrics. 2004 May;113(5):e385-94. doi: 10.1542/peds.113.5.e385. Pediatrics. 2004. PMID: 15121979
-
How pediatricians in Spain manage the first acute wheezing episode in an atopic infant. Results from the TRAP study.Allergol Immunopathol (Madr). 2005 Nov-Dec;33(6):317-25. doi: 10.1016/s0301-0546(05)73250-x. Allergol Immunopathol (Madr). 2005. PMID: 16371219
-
Variations in management of common inpatient pediatric illnesses: hospitalists and community pediatricians.Pediatrics. 2006 Aug;118(2):441-7. doi: 10.1542/peds.2006-0484. Pediatrics. 2006. PMID: 16882793
-
Pediatrician and family physician prescription of selective serotonin reuptake inhibitors.Pediatrics. 2000 Jun;105(6):E82. doi: 10.1542/peds.105.6.e82. Pediatrics. 2000. PMID: 10835095
Cited by
-
Intimate partner violence exposure, salivary cortisol, and childhood asthma.Child Abuse Negl. 2012 Jul-Aug;36(7-8):596-601. doi: 10.1016/j.chiabu.2011.12.002. Epub 2012 Jul 31. Child Abuse Negl. 2012. PMID: 22858093 Free PMC article.
-
The Asthma Control and Communication Instrument: a clinical tool developed for ethnically diverse populations.J Allergy Clin Immunol. 2008 Nov;122(5):936-943.e6. doi: 10.1016/j.jaci.2008.08.027. Epub 2008 Oct 11. J Allergy Clin Immunol. 2008. PMID: 18848721 Free PMC article.
-
Validation of parental reports of asthma trajectory, burden, and risk by using the pediatric asthma control and communication instrument.J Allergy Clin Immunol Pract. 2014 Mar-Apr;2(2):186-92. doi: 10.1016/j.jaip.2013.10.005. Epub 2014 Jan 17. J Allergy Clin Immunol Pract. 2014. PMID: 24607047 Free PMC article.
-
Translation and cultural adaptation of a specific instrument for measuring asthma control and asthma status: the Asthma Control and Communication Instrument.J Bras Pneumol. 2017 Jul-Aug;43(4):264-269. doi: 10.1590/S1806-37562016000000182. J Bras Pneumol. 2017. PMID: 29365000 Free PMC article.
-
Pediatrician qualifications and asthma management behaviors and their association with patient race/ethnicity.J Asthma. 2014 Mar;51(2):155-61. doi: 10.3109/02770903.2013.860163. Epub 2013 Dec 6. J Asthma. 2014. PMID: 24256071 Free PMC article.
References
-
- National Asthma Education and Prevention Program. Expert panel report: guidelines for the diagnosis and management of asthma—update on selected topics: 2002. J Allergy Clin Immunol. 2002;110(5 suppl):S142–S219. - PubMed
-
- Patino CM, Riekert KA, Quartey RI. Howard-Hopkins Center for Reducing Asthma Disparities. Development of the Asthma Control and Communication Instrument (ACCI) Am J Respir Crit Care Med. 2005;2:A254.
-
- Asch DA, Jedrziewski MK, Christakis NA. Response rates to mail surveys published in medical journals. J Clin Epidemiol. 1997;50(10):1129–1136. - PubMed
-
- Walter SD, Cook DJ. Confidence in life-support decisions in the intensive care unit: a survey of healthcare workers. Canadian Critical Care Trials Group. Crit Care Med. 1998;26(1):44–49. - PubMed
