

Consistent aspirin use associated with improved arteriovenous fistula survival among incident hemodialysis patients in the dialysis outcomes and practice patterns study
- PMID: 18596119
- PMCID: PMC2518799
- DOI: 10.2215/CJN.00130108
Consistent aspirin use associated with improved arteriovenous fistula survival among incident hemodialysis patients in the dialysis outcomes and practice patterns study
Abstract
Background and objectives: The relationship between aspirin use and arteriovenous fistula (AVF) survival has been lacking. The aim of this study was to evaluate the association between AVF survival and aspirin use.
Design, setting, participants, & measurements: Data on 2815 incident hemodialysis patients (on dialysis <or= 30 d) using an AVF at enrollment into the Dialysis Outcomes and Practice Patterns Study between 1996 and 2004 were analyzed. Cox regression was used to examine the association between aspirin use and the risk of final AVF failure, first AVF failure, and a gastrointestinal bleeding event. Aspirin use was determined at baseline and one year later. Patients using aspirin at baseline and one year later were considered consistent aspirin users. All models accounted for facility clustering effects and were adjusted for age, race, gender, body mass index, prior permanent access failure, prior placement of a catheter, 10 comorbid conditions, laboratory data, and other medications, and stratified by regions.
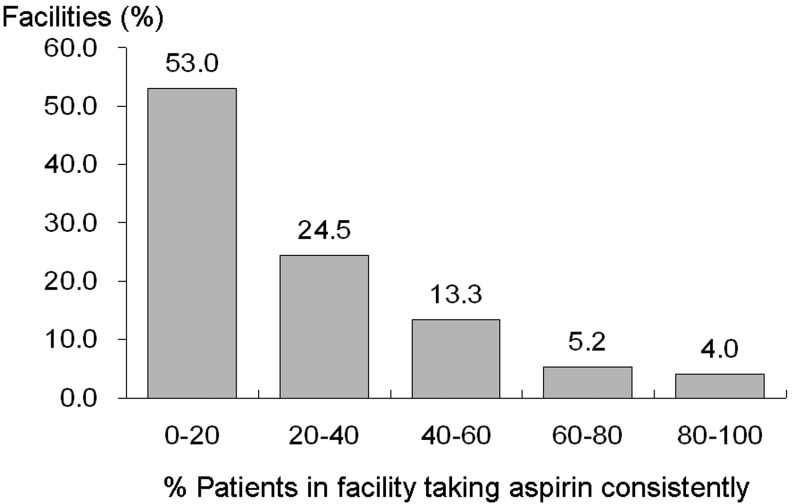
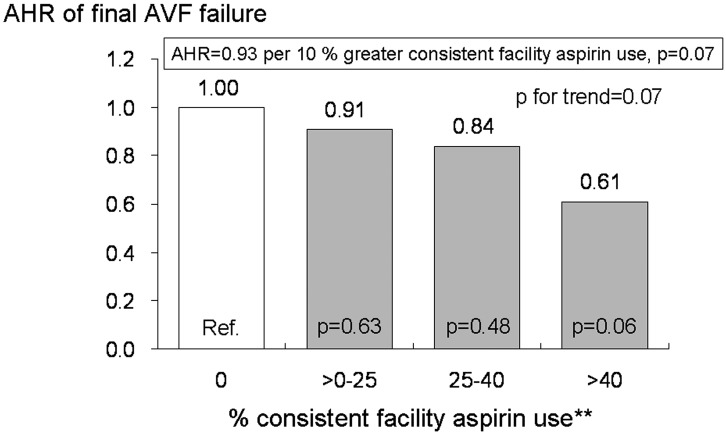
Results: Consistent aspirin use was significantly related to a lower risk of final AVF failure. Facility-level analysis, which may reduce confounding by indication, also showed a nearly significant trend of reduced risk of final AVF failure with greater prevalence of consistent aspirin use within dialysis facilities (P for trend = 0.07). The occurrence of a new gastrointestinal bleeding event during the study period was not associated with aspirin use.
Conclusions: These results suggest that consistent aspirin use may be beneficial for AVF survival among incident hemodialysis patients.
Figures

Similar articles
-
International Comparisons of Native Arteriovenous Fistula Patency and Time to Becoming Catheter-Free: Findings From the Dialysis Outcomes and Practice Patterns Study (DOPPS).Am J Kidney Dis. 2021 Feb;77(2):245-254. doi: 10.1053/j.ajkd.2020.06.020. Epub 2020 Sep 21. Am J Kidney Dis. 2021. PMID: 32971192
-
Preventing arteriovenous shunt failure in hemodialysis patients: a population-based cohort study.J Thromb Haemost. 2019 Jan;17(1):77-87. doi: 10.1111/jth.14347. Epub 2018 Dec 24. J Thromb Haemost. 2019. PMID: 30472783
-
Catheter Dependence After Arteriovenous Fistula or Graft Placement Among Elderly Patients on Hemodialysis.Am J Kidney Dis. 2021 Sep;78(3):399-408.e1. doi: 10.1053/j.ajkd.2020.12.019. Epub 2021 Feb 12. Am J Kidney Dis. 2021. PMID: 33582176
-
Novel insights into modifiable risk factors for arteriovenous fistula failure and the importance of CKD lipid profile: A meta-analysis.J Vasc Access. 2024 Sep;25(5):1416-1431. doi: 10.1177/11297298221115557. Epub 2023 Mar 23. J Vasc Access. 2024. PMID: 36951426
-
Pre-existing arterial pathologic changes affecting arteriovenous fistula patency and cardiovascular mortality in hemodialysis patients.Korean J Intern Med. 2017 Sep;32(5):790-797. doi: 10.3904/kjim.2017.268. Epub 2017 Aug 22. Korean J Intern Med. 2017. PMID: 28823140 Free PMC article. Review.
Cited by
-
Effects of aspirin resistance and mean platelet volume on vascular access failure in hemodialysis patients.Korean J Intern Med. 2019 Nov;34(6):1304-1312. doi: 10.3904/kjim.2018.111. Epub 2018 Jul 23. Korean J Intern Med. 2019. PMID: 30025441 Free PMC article.
-
Thrombophilia and arteriovenous fistula survival in ESRD.Clin J Am Soc Nephrol. 2013 Jun;8(6):962-8. doi: 10.2215/CJN.03860412. Epub 2013 Feb 14. Clin J Am Soc Nephrol. 2013. PMID: 23411429 Free PMC article.
-
Low-Dose Aspirin Use Significantly Improves the Survival of Late-stage NPC: A Propensity Score-Matched Cohort Study in Taiwan.Cancers (Basel). 2020 Jun 12;12(6):1551. doi: 10.3390/cancers12061551. Cancers (Basel). 2020. PMID: 32545461 Free PMC article.
-
Continuous aspirin treatment improves cardiovascular events and all-cause mortality in hemodialysis patients with peripheral artery disease.Ren Fail. 2024 Dec;46(2):2380754. doi: 10.1080/0886022X.2024.2380754. Epub 2024 Jul 22. Ren Fail. 2024. PMID: 39039846 Free PMC article.
-
The Effect of Antiplatelet Drugs on the Patency Rate of Arterio-venous Fistulae in Hemodialysis Patients.Iran J Pharm Res. 2010 Fall;9(4):451-7. Iran J Pharm Res. 2010. PMID: 24381612 Free PMC article.
References
-
- Hakim R, Himmelfarb J: Hemodialysis access failure: a call to action. Kidney Int 54 :1029 –1040,1998 - PubMed
-
- Rodriguez JA, Armadans L, Ferrer E, Olmos A, Codina S, Bartolome J, Borrellas J, Piera L: The function of permanent vascular access. Nephrol Dial Transplant 15 :402 –408,2000 - PubMed
-
- Akiba T, Akizawa T, Fukuhara S, Saito A, Ohira S, Sekino H, Yamazaki C, Kishimoto T, Osawa G, Fujimi S, Marumo F, Kurokawa K, Bragg-Gresham JL, Pisoni RL, Port FK, Held PJ: Results of the international DOPPS hemodialysis study in Japan. J Jpn Soc Dial Ther 37 :1865 –1873,2004
-
- Pisoni RL, Young EW, Dykstra DM, Greenwood RN, Hecking E, Gillespie B, Wolfe RA, Goodkin DA, Held PJ: Vascular access use in Europe and the United States: results from the DOPPS. Kidney Int 61 :305 –316,2002 - PubMed
-
- Sands JJ: Increasing AV fistulae and decreasing dialysis catheters: two aspects of improving patient outcomes. Blood Purif 25 :99 –102,2007 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
