

Efficacy of parenteral nutrition supplemented with glutamine dipeptide to decrease hospital infections in critically ill surgical patients
- PMID: 18596310
- PMCID: PMC3062504
- DOI: 10.1177/0148607108317880
Efficacy of parenteral nutrition supplemented with glutamine dipeptide to decrease hospital infections in critically ill surgical patients
Abstract
Background: Nosocomial infections are an important cause of morbidity and mortality in the surgical intensive care unit (SICU). Clinical benefits of glutamine-supplemented parenteral nutrition may occur in hospitalized surgical patients, but efficacy data in different surgical subgroups are lacking. The objective was to determine whether glutamine-supplemented parenteral nutrition differentially affects nosocomial infection rates in selected subgroups of SICU patients.
Methods: This was a double-blind, randomized, controlled study of alanyl-glutamine dipeptide-supplemented parenteral nutrition in SICU patients requiring parenteral nutrition and SICU care after surgery for pancreatic necrosis, cardiac, vascular, or colonic surgery. Subjects (n = 59) received isocaloric/isonitrogenous parenteral nutrition, providing 1.5 g/kg/d standard glutamine-free amino acids (STD-PN) or 1.0 g/kg/d standard amino acids + 0.5 g/kg/d glutamine dipeptide (GLN-PN). Enteral feedings were advanced as tolerated. Nosocomial infections were determined until hospital discharge.
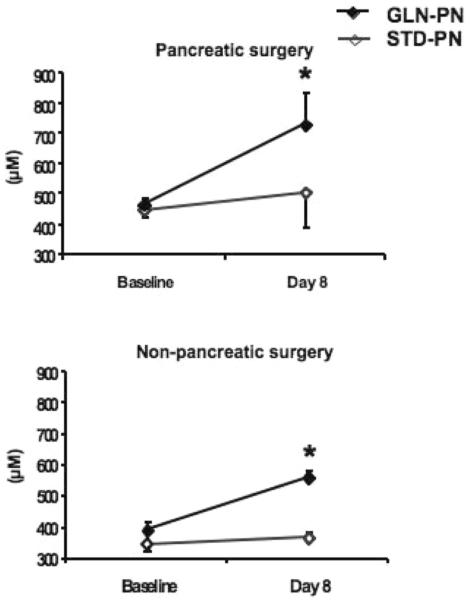
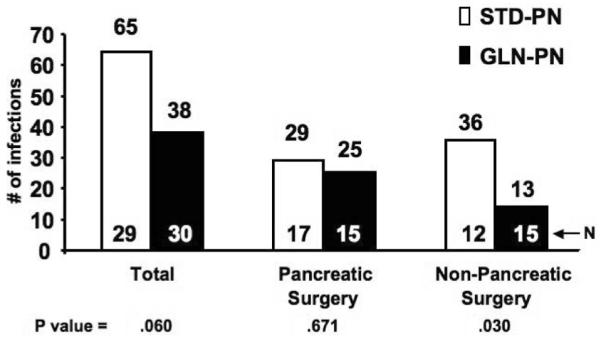
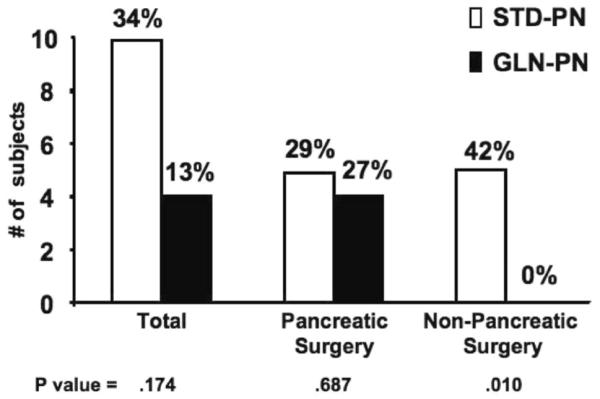
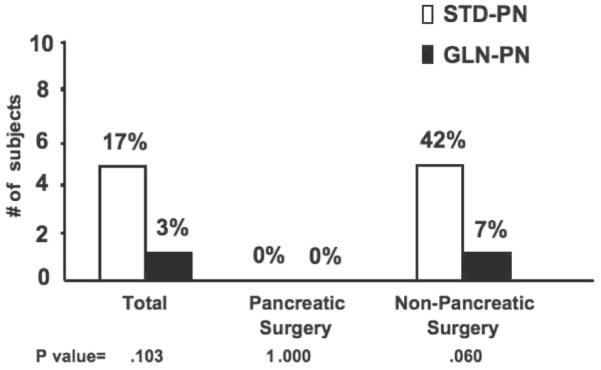
Results: Baseline clinical/metabolic data were similar between groups. Plasma glutamine concentrations were low in all groups and were increased by GLN-PN. GLN-PN did not alter infection rates after pancreatic necrosis surgery (17 STD-PN and 15 GLN-PN patients). In nonpancreatic surgery patients (12 STD-PN and 15 GLN-PN), GLN-PN was associated with significantly decreased total nosocomial infections (STD-PN 36 vs GLN-PN 13, P < .030), bloodstream infections (7 vs 0, P < .01), pneumonias (16 vs 6, P < .05), and infections attributed to Staphylococcus aureus (P < .01), fungi, and enteric Gram-negative bacteria (each P < .05).
Conclusions: Glutamine dipeptide-supplemented parenteral nutrition did not alter infection rates following pancreatic necrosis surgery but significantly decreased infections in SICU patients after cardiac, vascular, and colonic surgery.
Figures
References
-
- Vincent JL, Bihari DJ, Suter PM, et al. EPIC International Advisory Committee The prevalence of nosocomial infection in intensive care units in Europe: results of the European Prevalence of Infection in Intensive Care (EPIC) Study. JAMA. 1995;274:639–644. - PubMed
-
- Girou E, Stephan F, Novara A, Safar M, Fagon JY. Risk factors and outcome of nosocomial infections: results of a matched case-control study of ICU patients. Am J Respir Crit Care Med. 1998;157:1151–1158. - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348:1546–1554. - PubMed
-
- Richards MJ, Edwards JR, Culver DH, Gaynes RP. Nosocomial infections in combined medical-surgical intensive care units in the United States. Infect Control Hosp Epidemiol. 2000;21:510–515. - PubMed
-
- Salgado CD, O’Grady N, Farr BM. Prevention and control of antimicrobial-resistant infections in intensive care patients. Crit Care Med. 2005;33:2373–2382. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
