

Effective, robust design of community mitigation for pandemic influenza: a systematic examination of proposed US guidance
- PMID: 18596963
- PMCID: PMC2432023
- DOI: 10.1371/journal.pone.0002606
Effective, robust design of community mitigation for pandemic influenza: a systematic examination of proposed US guidance
Abstract
Background: The US government proposes pandemic influenza mitigation guidance that includes isolation and antiviral treatment of ill persons, voluntary household member quarantine and antiviral prophylaxis, social distancing of individuals, school closure, reduction of contacts at work, and prioritized vaccination. Is this the best strategy combination? Is choice of this strategy robust to pandemic uncertainties? What are critical enablers of community resilience?
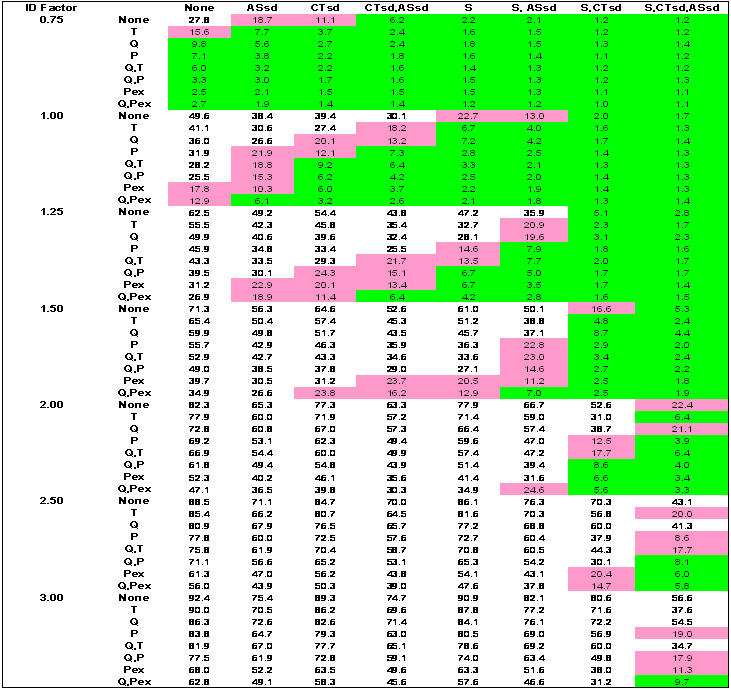
Methods and findings: We systematically simulate a broad range of pandemic scenarios and mitigation strategies using a networked, agent-based model of a community of explicit, multiply-overlapping social contact networks. We evaluate illness and societal burden for alterations in social networks, illness parameters, or intervention implementation. For a 1918-like pandemic, the best strategy minimizes illness to <1% of the population and combines network-based (e.g. school closure, social distancing of all with adults' contacts at work reduced), and case-based measures (e.g. antiviral treatment of the ill and prophylaxis of household members). We find choice of this best strategy robust to removal of enhanced transmission by the young, additional complexity in contact networks, and altered influenza natural history including extended viral shedding. Administration of age-group or randomly targeted 50% effective pre-pandemic vaccine with 7% population coverage (current US H5N1 vaccine stockpile) had minimal effect on outcomes. In order, mitigation success depends on rapid strategy implementation, high compliance, regional mitigation, and rigorous rescinding criteria; these are the critical enablers for community resilience.
Conclusions: Systematic evaluation of feasible, recommended pandemic influenza interventions generally confirms the US community mitigation guidance yields best strategy choices for pandemic planning that are robust to a wide range of uncertainty. The best strategy combines network- and case-based interventions; network-based interventions are paramount. Because strategies must be applied rapidly, regionally, and stringently for greatest benefit, preparation and public education is required for long-lasting, high community compliance during a pandemic.
Conflict of interest statement
Figures





Similar articles
-
Effectiveness and cost-effectiveness of expanded antiviral prophylaxis and adjuvanted vaccination strategies for an influenza A (H5N1) pandemic.Ann Intern Med. 2009 Dec 15;151(12):840-53. doi: 10.7326/0003-4819-151-12-200912150-00156. Ann Intern Med. 2009. PMID: 20008760 Free PMC article.
-
Rescinding community mitigation strategies in an influenza pandemic.Emerg Infect Dis. 2008 Mar;14(3):365-72. doi: 10.3201/eid1403.070673. Emerg Infect Dis. 2008. PMID: 18325247 Free PMC article.
-
Community Mitigation Guidelines to Prevent Pandemic Influenza - United States, 2017.MMWR Recomm Rep. 2017 Apr 21;66(1):1-34. doi: 10.15585/mmwr.rr6601a1. MMWR Recomm Rep. 2017. PMID: 28426646 Free PMC article.
-
The risk of seasonal and pandemic influenza: prospects for control.Clin Infect Dis. 2009 Jan 1;48 Suppl 1:S20-5. doi: 10.1086/591853. Clin Infect Dis. 2009. PMID: 19067611 Review.
-
Non-pharmaceutical public health interventions for pandemic influenza: an evaluation of the evidence base.BMC Public Health. 2007 Aug 15;7:208. doi: 10.1186/1471-2458-7-208. BMC Public Health. 2007. PMID: 17697389 Free PMC article. Review.
Cited by
-
Selection of key recommendations for quality indicators describing good quality outbreak response.BMC Infect Dis. 2015 Mar 31;15:166. doi: 10.1186/s12879-015-0896-x. BMC Infect Dis. 2015. PMID: 25888491 Free PMC article.
-
Evidence-based tool for triggering school closures during influenza outbreaks, Japan.Emerg Infect Dis. 2009 Nov;15(11):1841-3. doi: 10.3201/eid1511.090798. Emerg Infect Dis. 2009. PMID: 19891880 Free PMC article.
-
Economic and social impact of influenza mitigation strategies by demographic class.Epidemics. 2011 Mar;3(1):19-31. doi: 10.1016/j.epidem.2010.11.002. Epidemics. 2011. PMID: 21339828 Free PMC article.
-
Social network sensors for early detection of contagious outbreaks.PLoS One. 2010 Sep 15;5(9):e12948. doi: 10.1371/journal.pone.0012948. PLoS One. 2010. PMID: 20856792 Free PMC article.
-
Vaccination strategies for future influenza pandemics: a severity-based cost effectiveness analysis.BMC Infect Dis. 2013 Feb 11;13:81. doi: 10.1186/1471-2334-13-81. BMC Infect Dis. 2013. PMID: 23398722 Free PMC article.
References
-
- McCaw JM, McVernon J. Prophylaxis or treatment? Optimal use of an antiviral stockpile during an influenza pandemic. Math Biosci. 2007;209:336–360. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
