

On the prevalence of M. avium subspecies paratuberculosis DNA in the blood of healthy individuals and patients with inflammatory bowel disease
- PMID: 18596984
- PMCID: PMC2434204
- DOI: 10.1371/journal.pone.0002537
On the prevalence of M. avium subspecies paratuberculosis DNA in the blood of healthy individuals and patients with inflammatory bowel disease
Abstract
Background: Mycobacteria, such as M. leprae and M. tuberculosis infect billions of humans. However, because of appropriate immune responses and antibiotic therapy, overt mycobacterial diseases occur far less frequently. M. avium subspecies paratuberculosis (MAP) causes Johne's disease in ruminants, an affliction evocative of inflammatory bowel disease (IBD). Several agents used to treat IBD (5-ASA, methotrexate, azathioprine and its metabolite 6-MP) have recently been shown to be antiMAP antibiotics. We herein evaluate the prevalence of MAP DNA in healthy individuals and compare them with IBD patients on antiMAP antibiotics.
Methods: We studied 100 healthy individuals (90 blood donors) and 246 patients with IBD. IS900 MAP DNA was identified using a nested primer PCR in the buffy coat of blood. Positive signal was confirmed as MAP by DNA sequence analysis. PCR positive results frequencies were compared according to medications used. Significance was accepted at p<0.05.
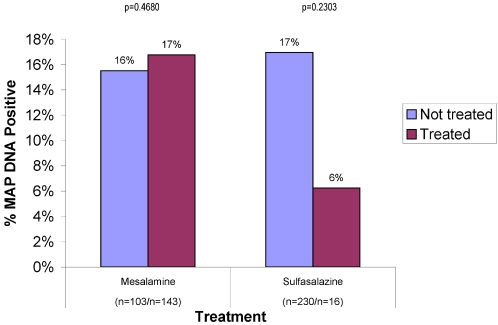
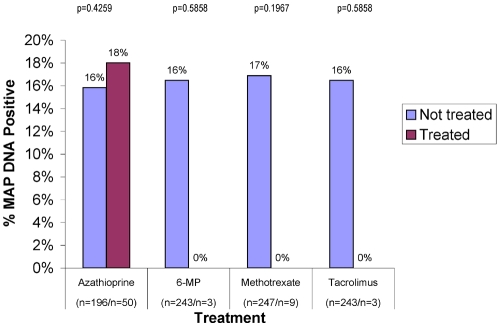
Results: 47% (47/100) healthy controls and 16% (40/246) IBD patients were IS900 positive (p<0.0001). MAP DNA was identified in 17% of 143 patients receiving mesalamine and 6% of 16 receiving sulfasalazine. None of the IBD patients receiving methotrexate (n = 9), 6-MP (n = 3), ciprofloxacin (n = 5) or Tacrolimus (n = 3) had MAP DNA detectable in their blood.
Discussion: We found a disquietingly large percentage of healthy individuals have MAP DNA in their blood, the significance of which remains to be determined. Counter-intuitively, the incidence of MAP DNA was significantly lower in patients with IBD. Agents with the most potent in vitro antiMAP activity were associated with clearance of blood MAP DNA. We posit that the use antiMAP antibiotics was responsible for the decreased prevalence of MAP DNA in patients with IBD.
Conflict of interest statement
Figures



Similar articles
-
Paucity of mycobacteria in mucosal bowel biopsies from adults and children with early inflammatory bowel disease.J Crohns Colitis. 2010 Nov;4(5):561-6. doi: 10.1016/j.crohns.2010.05.003. Epub 2010 Jun 18. J Crohns Colitis. 2010. PMID: 21122560
-
Results of multiple diagnostic tests for Mycobacterium avium subsp. paratuberculosis in patients with inflammatory bowel disease and in controls.J Clin Microbiol. 2000 Dec;38(12):4373-81. doi: 10.1128/JCM.38.12.4373-4381.2000. J Clin Microbiol. 2000. PMID: 11101567 Free PMC article.
-
Association between Mycobacterium avium subsp. paratuberculosis DNA in blood and cellular and humoral immune response in inflammatory bowel disease patients and controls.Int J Infect Dis. 2009 Mar;13(2):247-54. doi: 10.1016/j.ijid.2008.06.034. Epub 2008 Oct 15. Int J Infect Dis. 2009. PMID: 18922720
-
Is Crohn's disease caused by a mycobacterium? Comparisons with leprosy, tuberculosis, and Johne's disease.Lancet Infect Dis. 2003 Aug;3(8):507-14. doi: 10.1016/s1473-3099(03)00724-2. Lancet Infect Dis. 2003. PMID: 12901893 Review.
-
Advances in epidemiology and diagnosis of inflammatory bowel diseases.Curr Gastroenterol Rep. 2008 Dec;10(6):576-84. doi: 10.1007/s11894-008-0105-9. Curr Gastroenterol Rep. 2008. PMID: 19006614 Review.
Cited by
-
Anti-inflammatory and antiapoptotic responses to infection: a common denominator of human and bovine macrophages infected with Mycobacterium avium subsp. paratuberculosis.Biomed Res Int. 2013;2013:908348. doi: 10.1155/2013/908348. Epub 2013 Jan 20. Biomed Res Int. 2013. PMID: 23509800 Free PMC article. Review.
-
Presence of intestinal Mycobacterium avium subspecies paratuberculosis (MAP) DNA is not associated with altered MMP expression in ulcerative colitis.BMC Gastroenterol. 2011 Apr 8;11:34. doi: 10.1186/1471-230X-11-34. BMC Gastroenterol. 2011. PMID: 21477272 Free PMC article.
-
Crohn's disease: evidence for involvement of unregulated transcytosis in disease etio-pathogenesis.World J Gastroenterol. 2011 Mar 21;17(11):1416-26. doi: 10.3748/wjg.v17.i11.1416. World J Gastroenterol. 2011. PMID: 21472099 Free PMC article. Review.
-
Evaluation of "Indigenous Absorbed ELISA Kit" for the Estimation of Seroprevalence of Mycobacterium avium Subspecies paratuberculosis Antibodies in Human Beings in North India.ISRN Vet Sci. 2011 May 23;2011:636038. doi: 10.5402/2011/636038. Print 2011. ISRN Vet Sci. 2011. PMID: 23738105 Free PMC article.
-
Alteration of Gut Microbiota in Inflammatory Bowel Disease (IBD): Cause or Consequence? IBD Treatment Targeting the Gut Microbiome.Pathogens. 2019 Aug 13;8(3):126. doi: 10.3390/pathogens8030126. Pathogens. 2019. PMID: 31412603 Free PMC article. Review.
References
-
- Ramaprasad P, Fernando A, Madhale S, Rao JR, Edward VK, et al. Transmission and protection in leprosy: indications of the role of mucosal immunity. Lepr Rev. 1997;68:301–315. - PubMed
-
- Britton WJ, Lockwood DN. Leprosy. Lancet. 2004;363:1209–1219. - PubMed
-
- 2003 WHO annual report on global TB control–summary. Wkly Epidemiol Rec. 78:122–128. - PubMed
-
- Corbett EL, Watt CJ, Walker N, Maher D, Williams BG, et al. The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. Arch Intern Med. 2003;163:1009–1021. - PubMed
-
- Johne HA, Frothingham L. Ein eigenthumlicher fall von tuberculose beim rind ( A particular case of tuberculosis in a cow). Dtsch Zeitschr Tiermed, Vergl Pathol. 1895;21:438–454.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
