

Shedding of live vaccine virus, comparative safety, and influenza-specific antibody responses after administration of live attenuated and inactivated trivalent influenza vaccines to HIV-infected children
- PMID: 18597900
- PMCID: PMC2615200
- DOI: 10.1016/j.vaccine.2008.05.054
Shedding of live vaccine virus, comparative safety, and influenza-specific antibody responses after administration of live attenuated and inactivated trivalent influenza vaccines to HIV-infected children
Abstract
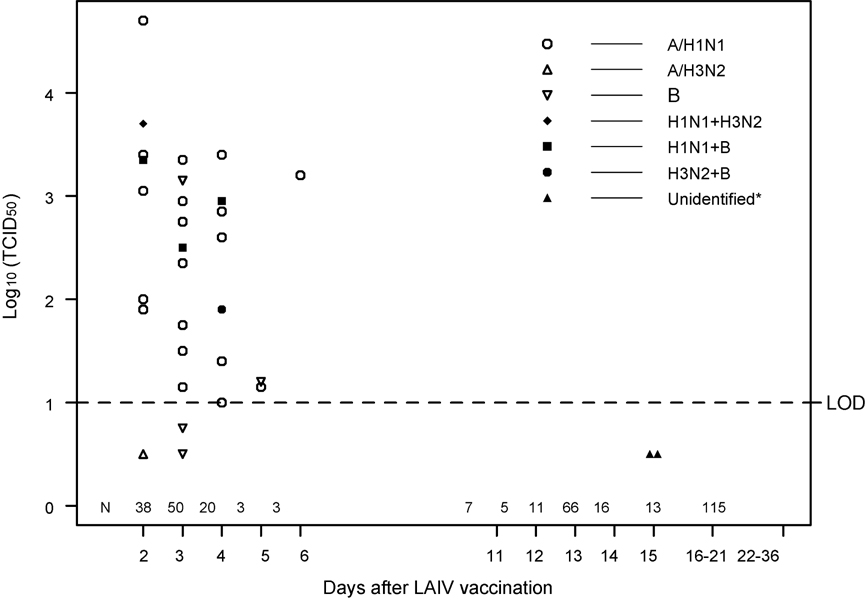
HIV-infected children (N=243), >or=5 to <18 years old, receiving stable antiretroviral therapy, were stratified by immunologic status and randomly assigned to receive intranasal live attenuated influenza vaccine (LAIV) or intramuscular trivalent inactivated influenza vaccine (TIV). The safety profile after LAIV or TIV closely resembled the previously reported tolerability to these vaccines in children without HIV infection. Post-vaccination hemagglutination inhibition (HAI) antibody responses and shedding of LAIV virus were also similar, regardless of immunological stratum, to antibody responses and shedding previously reported for children without HIV infection. LAIV should be further evaluated for a role in immunizing HIV-infected children.
Figures
References
-
- Morishima T, Togashi T, Yogata S, et al. Encephalitis and encephalopathy associated with an influenza epidemic in Japan. Clin Infect Dis. 2002;35:512–517. - PubMed
-
- Siberry GK. Complications of influenza infection in children. Pediatric Annals. 2000;209:683–690. - PubMed
-
- Neuzil KM, Zhu Y, Griffin MR, et al. Burden of interpandemic influenza in children younger than 5 years: a 25-year prospective study. J Infect Dis. 2002;185:147–152. - PubMed
-
- CDC. Prevention and control of influenza: recommendations of the Advisory Committee on Immmunization Practices (ACIP) MMWR. 2004;53(No RR6):1–40. - PubMed
-
- Rojo J, Ruiz-Contreras J, Fernandez M, Marin M, Folgueira I. Influenza-related hospitalizations in children younger than three years of age. Ped Infect Dis J. 2006;25:596–601. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
