

Case of yellow fever vaccine--associated viscerotropic disease with prolonged viremia, robust adaptive immune responses, and polymorphisms in CCR5 and RANTES genes
- PMID: 18598196
- PMCID: PMC3734802
- DOI: 10.1086/590187
Case of yellow fever vaccine--associated viscerotropic disease with prolonged viremia, robust adaptive immune responses, and polymorphisms in CCR5 and RANTES genes
Abstract
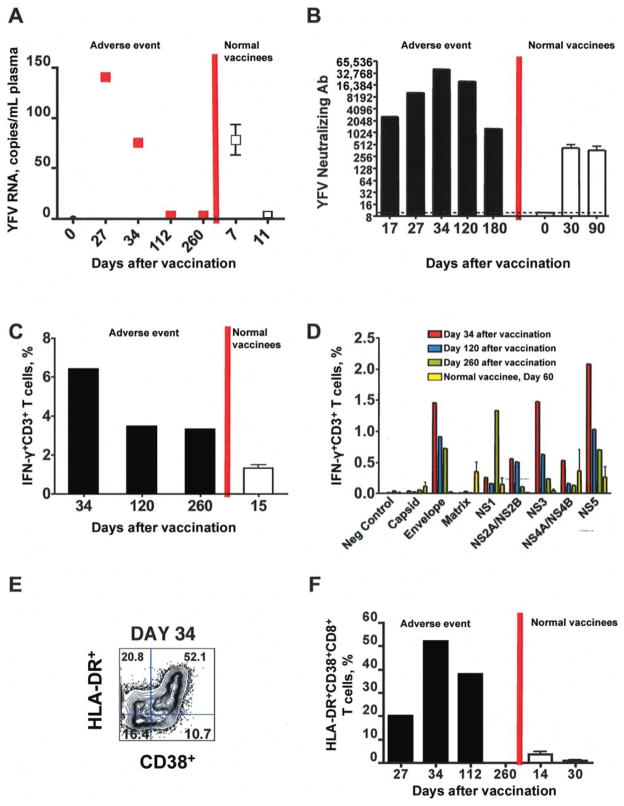
Background: The live attenuated yellow fever vaccine 17D (YF-17D) is one of the most effective vaccines. Despite its excellent safety record, some cases of viscerotropic adverse events develop, which are sometimes fatal. The mechanisms underlying such events remain a mystery. Here, we present an analysis of the immunologic and genetic factors driving disease in a 64-year-old male who developed viscerotropic symptoms.
Methods: We obtained clinical, serologic, virologic, immunologic and genetic data on this case patient.
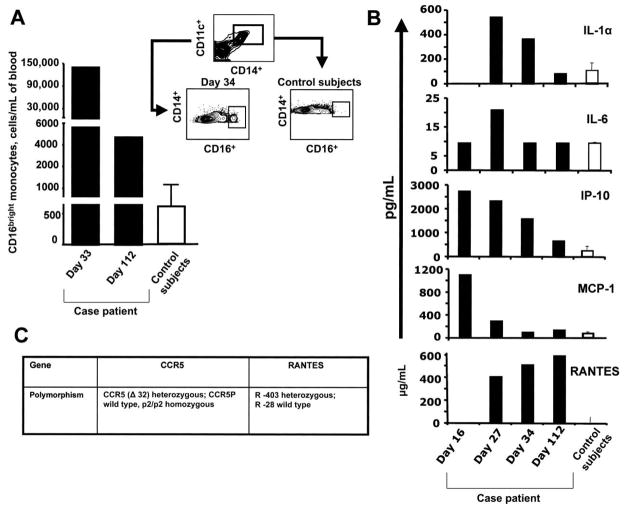
Results: Viral RNA was detected in the blood 33 days after vaccination, in contrast to the expected clearance of virus by day 7 after vaccination in healthy vaccinees. Vaccination induced robust antigen-specific T and B cell responses, which suggested that persistent virus was not due to adaptive immunity of suboptimal magnitude. The genes encoding OAS1, OAS2, TLR3, and DC-SIGN, which mediate antiviral innate immunity, were wild type. However, there were heterozygous genetic polymorphisms in chemokine receptor CCR5, and its ligand RANTES, which influence the migration of effector T cells and CD14+CD16bright monocytes to tissues. Consistent with this, there was a 200-fold increase in the number of CD14+CD16bright monocytes in the blood during viremia and even several months after virus clearance.
Conclusion: In this patient, viscerotropic disease was not due to the impaired magnitude of adaptive immunity but instead to anomalies in the innate immune system and a possible disruption of the CCR5-RANTES axis.
Conflict of interest statement
Figures
Comment in
-
Response to "Case of yellow fever vaccine-associated viscerotropic disease with prolonged viremia, robust adaptive immune responses, and polymorphisms in CCR5 and RANTES genes".J Infect Dis. 2009 Feb 15;199(4):601. doi: 10.1086/596209. J Infect Dis. 2009. PMID: 19281308 No abstract available.
References
-
- Monath TP. Milestones in the conquest of yellow fever. In: Koprowski H, Oldstone MBA, editors. Microbe hunters: then and now. Lansing, MI: Medi-Ed Press; 1996. pp. 95–112.
-
- Pugachev KV, Guirakhoo F, Monath TP. New developments in flavivirus vaccines with special attention to yellow fever. Curr Opin Infect Dis. 2005;18:387–94. - PubMed
-
- Monath TP. Yellow fever vaccine. Expert Rev Vaccines. 2005;4:553–74. - PubMed
-
- Khromava AY, Eidex RB, Weld LH, et al. Yellow fever vaccine: an updated assessment of advanced age as a risk factor for serious adverse events. Vaccine. 2005;23:3256–63. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
