

Attributable outcomes of endemic Clostridium difficile-associated disease in nonsurgical patients
- PMID: 18598621
- PMCID: PMC2600322
- DOI: 10.3201/eid1407.070867
Attributable outcomes of endemic Clostridium difficile-associated disease in nonsurgical patients
Abstract
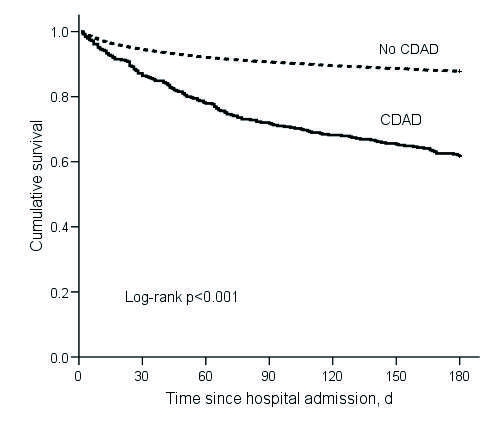
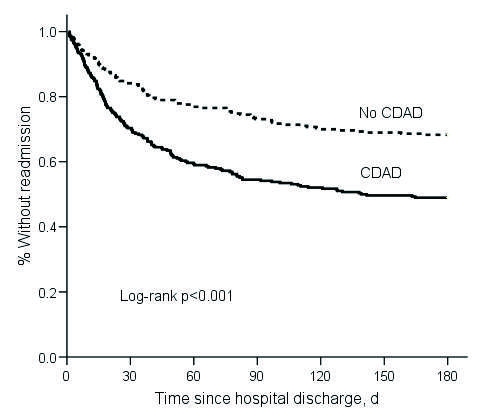
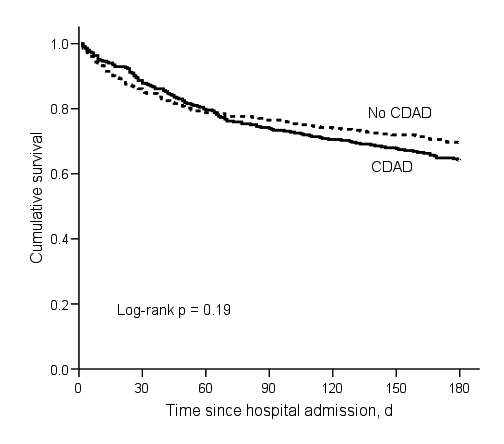
Data are limited on the attributable outcomes of Clostridium difficile-associated disease (CDAD), particularly in CDAD-endemic settings. We conducted a retrospective cohort study of nonsurgical inpatients admitted for >/=48 hours in 2003 (N = 18,050). The adjusted hazard ratios for readmission (hazard ratio 2.19, 95% confidence interval [CI] 1.87-2.55) and deaths within 180 days (hazard ratio 1.23, 95% CI 1.03-1.46) were significantly different among CDAD case-patients and noncase patients. In a propensity score matched-pairs analysis that used a nested subset of the cohort (N = 706), attributable length of stay attributable to CDAD was 2.8 days, attributable readmission at 180 days was 19.3%, and attributable death at 180 days was 5.7%. CDAD patients were significantly more likely than controls to be discharged to a long-term-care facility or outside hospital. Even in a nonoutbreak setting, CDAD had a statistically significant negative impact on patient illness and death, and the impact of CDAD persisted beyond hospital discharge.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical