

Proinflammatory cytokines oppose opioid-induced acute and chronic analgesia
- PMID: 18599265
- PMCID: PMC2783238
- DOI: 10.1016/j.bbi.2008.05.004
Proinflammatory cytokines oppose opioid-induced acute and chronic analgesia
Abstract
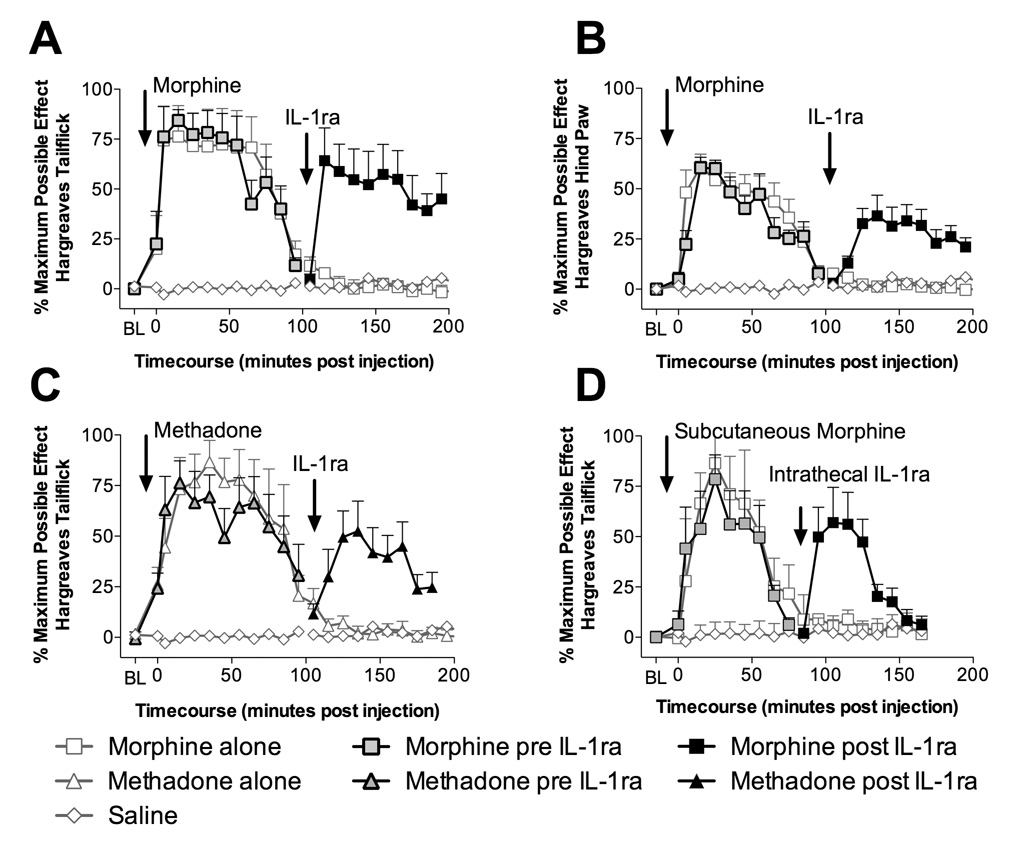
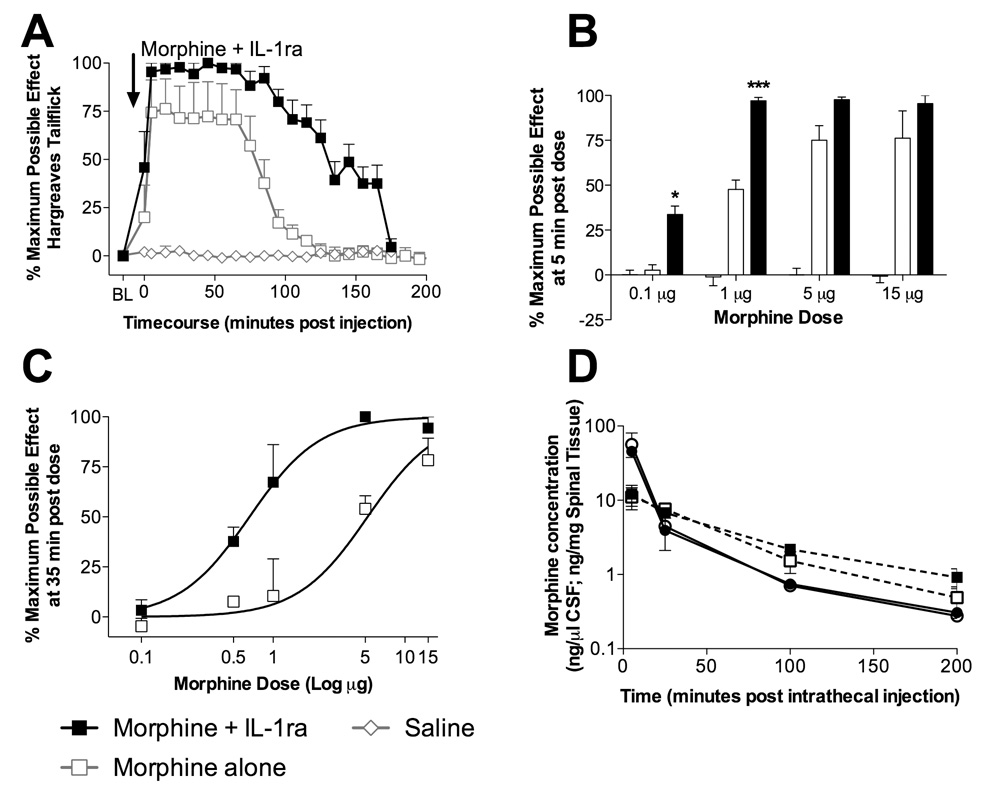
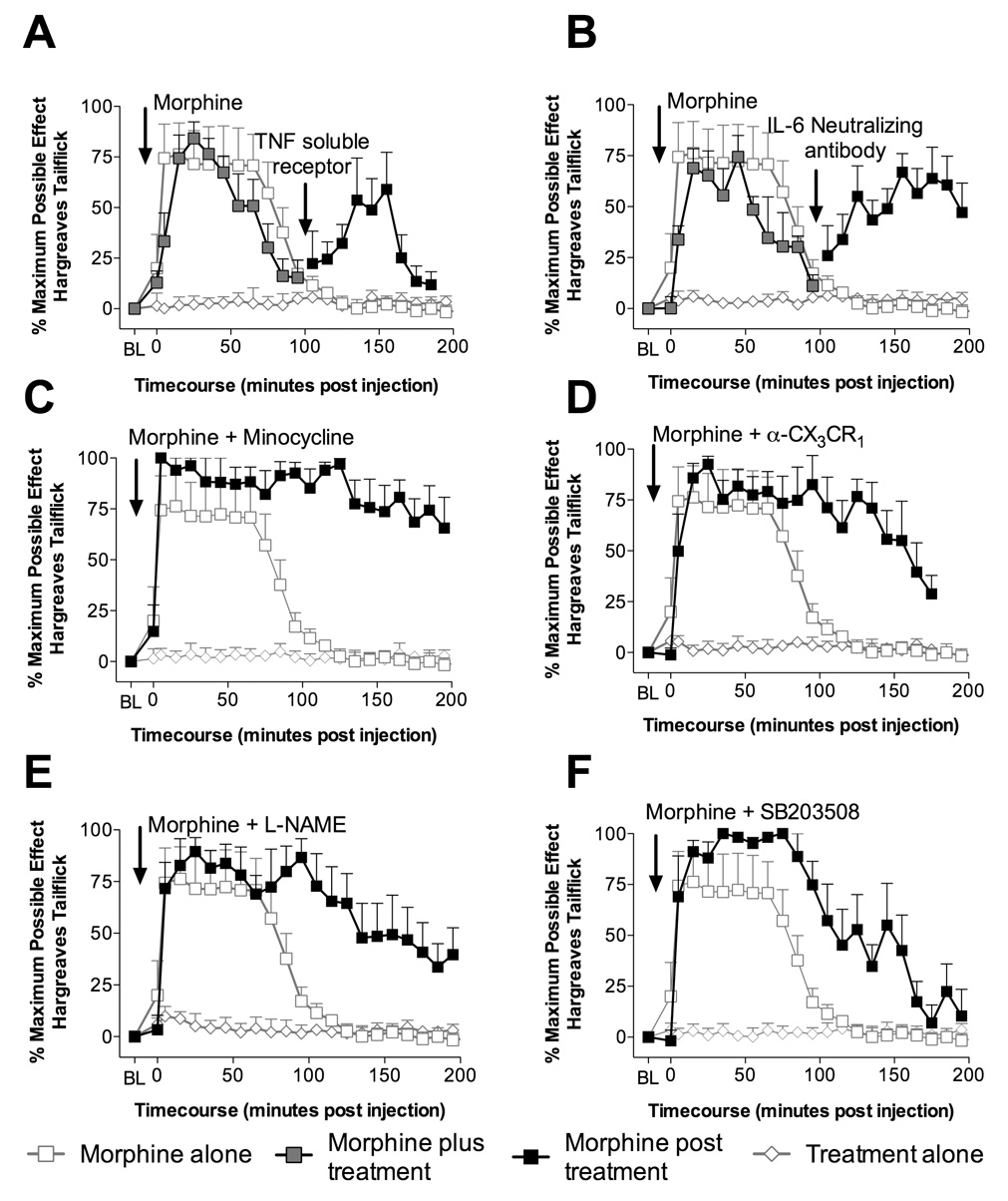
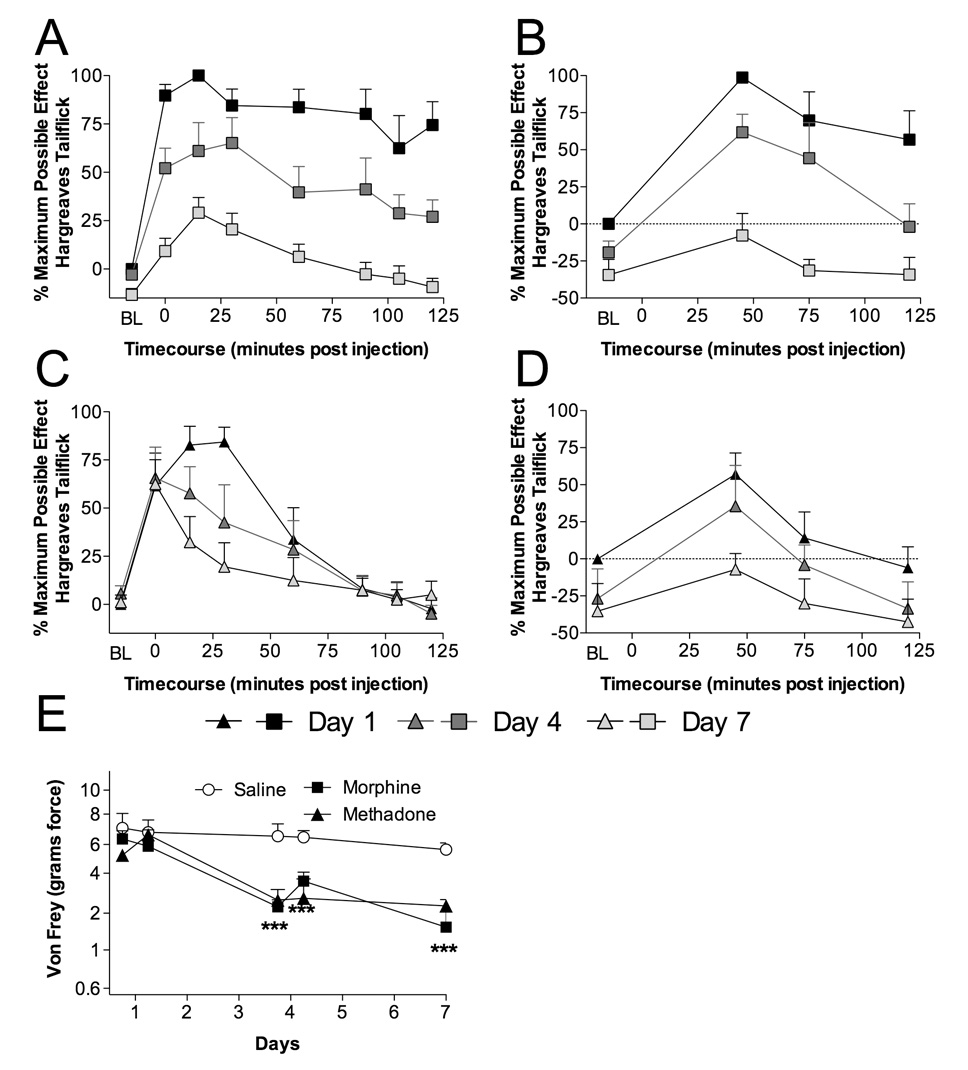
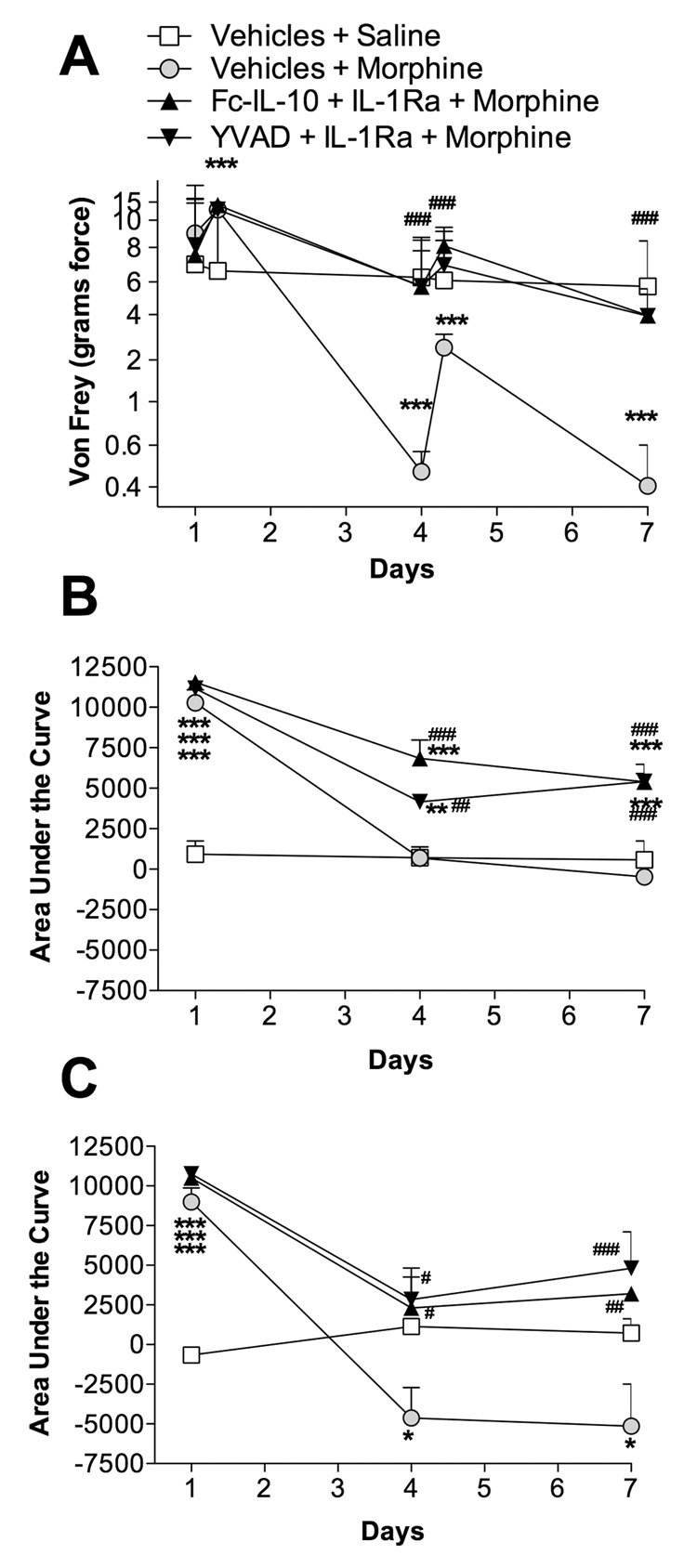
Spinal proinflammatory cytokines are powerful pain-enhancing signals that contribute to pain following peripheral nerve injury (neuropathic pain). Recently, one proinflammatory cytokine, interleukin-1, was also implicated in the loss of analgesia upon repeated morphine exposure (tolerance). In contrast to prior literature, we demonstrate that the action of several spinal proinflammatory cytokines oppose systemic and intrathecal opioid analgesia, causing reduced pain suppression. In vitro morphine exposure of lumbar dorsal spinal cord caused significant increases in proinflammatory cytokine and chemokine release. Opposition of analgesia by proinflammatory cytokines is rapid, occurring < or =5 min after intrathecal (perispinal) opioid administration. We document that opposition of analgesia by proinflammatory cytokines cannot be accounted for by an alteration in spinal morphine concentrations. The acute anti-analgesic effects of proinflammatory cytokines occur in a p38 mitogen-activated protein kinase and nitric oxide dependent fashion. Chronic intrathecal morphine or methadone significantly increased spinal glial activation (toll-like receptor 4 mRNA and protein) and the expression of multiple chemokines and cytokines, combined with development of analgesic tolerance and pain enhancement (hyperalgesia, allodynia). Statistical analysis demonstrated that a cluster of cytokines and chemokines was linked with pain-related behavioral changes. Moreover, blockade of spinal proinflammatory cytokines during a stringent morphine regimen previously associated with altered neuronal function also attenuated enhanced pain, supportive that proinflammatory cytokines are importantly involved in tolerance induced by such regimens. These data implicate multiple opioid-induced spinal proinflammatory cytokines in opposing both acute and chronic opioid analgesia, and provide a novel mechanism for the opposition of acute opioid analgesia.
Figures
References
-
- Carmody J. Avoiding fallacies in nociceptive measurements. Pain. 1995;63:136. - PubMed
-
- Chaplan SR, Bach FW, Pogrel JW, Chung JM, Yaksh TL. Quantitative assessment of tactile allodynia in the rat paw. J Neurosci Methods. 1994;53:55–63. - PubMed
-
- Cui Y, Chen Y, Zhi JL, Guo RX, Feng JQ, Chen PX. Activation of p38 mitogen-activated protein kinase in spinal microglia mediates morphine antinociceptive tolerance. Brain Res. 2006;1069:235–243. - PubMed
-
- Doverty M, Somogyi AA, White JM, Bochner F, Beare CH, Menelaou A, Ling W. Methadone maintenance patients are cross-tolerant to the antinociceptive effects of morphine. Pain. 2001;93:155–163. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
