

Viral reservoirs, residual viremia, and the potential of highly active antiretroviral therapy to eradicate HIV infection
- PMID: 18602567
- PMCID: PMC6812482
- DOI: 10.1016/j.jaci.2008.05.033
Viral reservoirs, residual viremia, and the potential of highly active antiretroviral therapy to eradicate HIV infection
Abstract
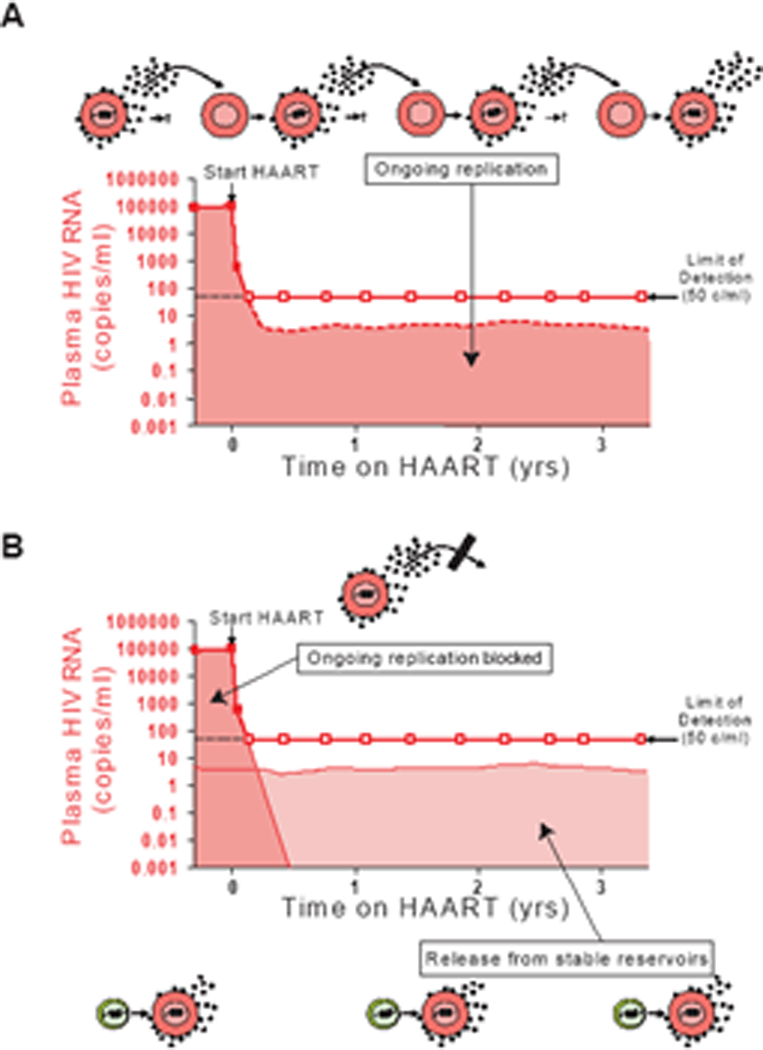
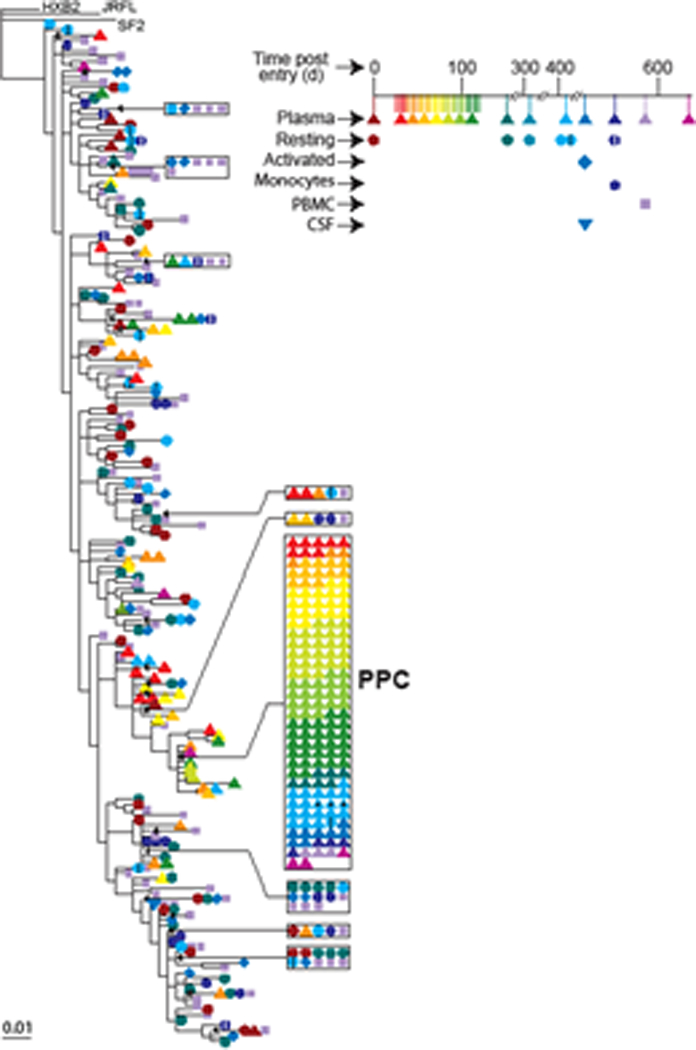
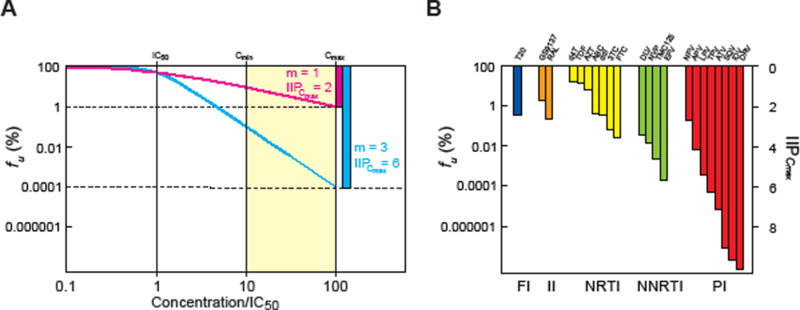
Although highly active antiretroviral therapy (HAART) can reduce HIV-1 viremia to levels that are below the limit of detection of clinical assays, the virus persists in reservoirs, and trace levels of free virions can be found in the plasma. Whether this residual viremia represents ongoing cycles of replication continuing despite HAART or simply the release of virus from stable reservoirs has been controversial. Here we summarize the evidence that HAART can stop ongoing cycles of replication. The evidence comes from a detailed analysis of the residual viremia, which shows it to be archival and nonevolving in character. In addition, new pharmacodynamic measures incorporating a previously ignored slope parameter have provided the first real indication of how well HAART actually suppresses viral replication in vivo. Together, these results argue that the ultimate theoretical potential of HAART to control viral replication has already been reached. Progress toward eradication of the infection will require novel approaches to target the stable reservoirs that persist even when viral replication is completely halted.
Figures
References
-
- Hammer SM, Squires KE, Hughes MD, Grimes JM, Demeter LM, Currier JS, et al. A controlled trial of two nucleoside analogues plus indinavir in persons with human immunodeficiency virus infection and CD4 cell counts of 200 per cubic millimeter or less. AIDS clinical trials group 320 study team. N Engl J Med 1997. September 11;337(11):725–33. - PubMed
-
- Gulick RM, Mellors JW, Havlir D, Eron JJ, Gonzalez C, McMahon D, et al. Treatment with indinavir, zidovudine, and lamivudine in adults with human immunodeficiency virus infection and prior antiretroviral therapy. N Engl J Med 1997. September 11;337(11):734–9. - PubMed
-
- Perelson AS, Essunger P, Cao Y, Vesanen M, Hurley A, Saksela K, et al. Decay characteristics of HIV-1-infected compartments during combination therapy. Nature 1997. May 8;387(6629):188–91. - PubMed
-
- Ho DD, Neumann AU, Perelson AS, Chen W, Leonard JM, Markowitz M. Rapid turnover of plasma virions and CD4 lymphocytes in HIV-1 infection. Nature 1995. January 12;373(6510):123–6. - PubMed
-
- Wei X, Ghosh SK, Taylor ME, Johnson VA, Emini EA, Deutsch P, et al. Viral dynamics in human immunodeficiency virus type 1 infection. Nature 1995. January 12;373(6510):117–22. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
