

Primary cardiac sarcomas: a clinicopathologic analysis of a series with follow-up information in 17 patients and emphasis on long-term survival
- PMID: 18602663
- PMCID: PMC4081532
- DOI: 10.1016/j.humpath.2008.01.019
Primary cardiac sarcomas: a clinicopathologic analysis of a series with follow-up information in 17 patients and emphasis on long-term survival
Abstract
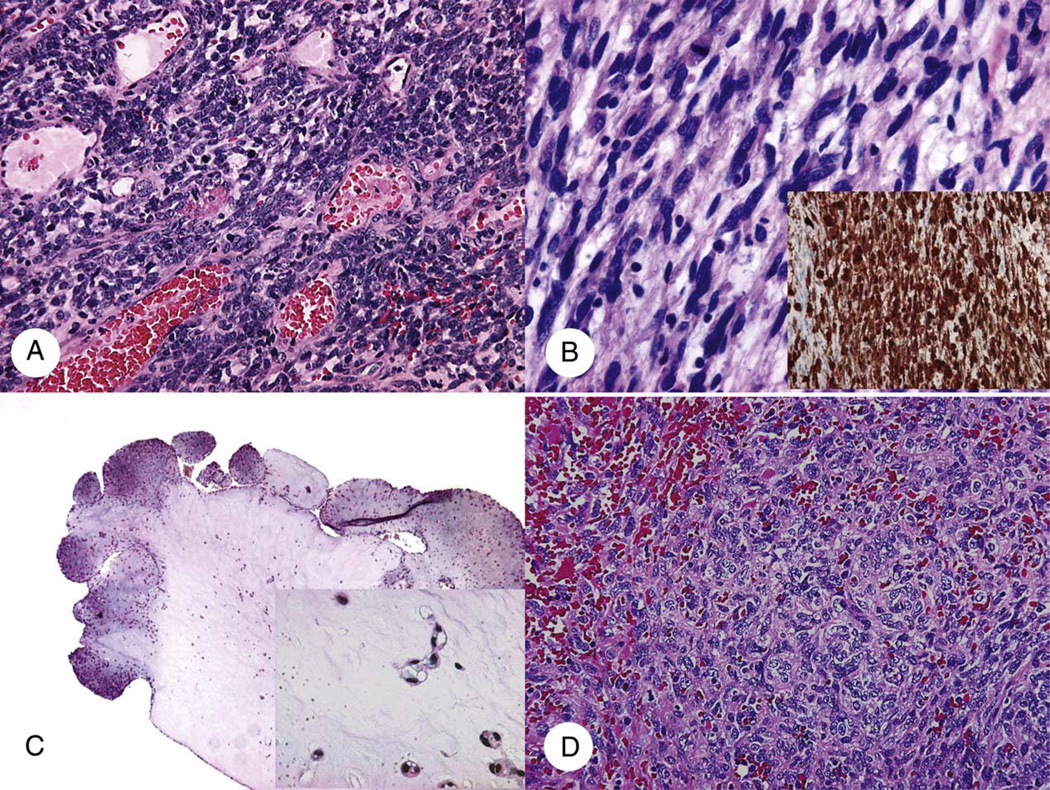
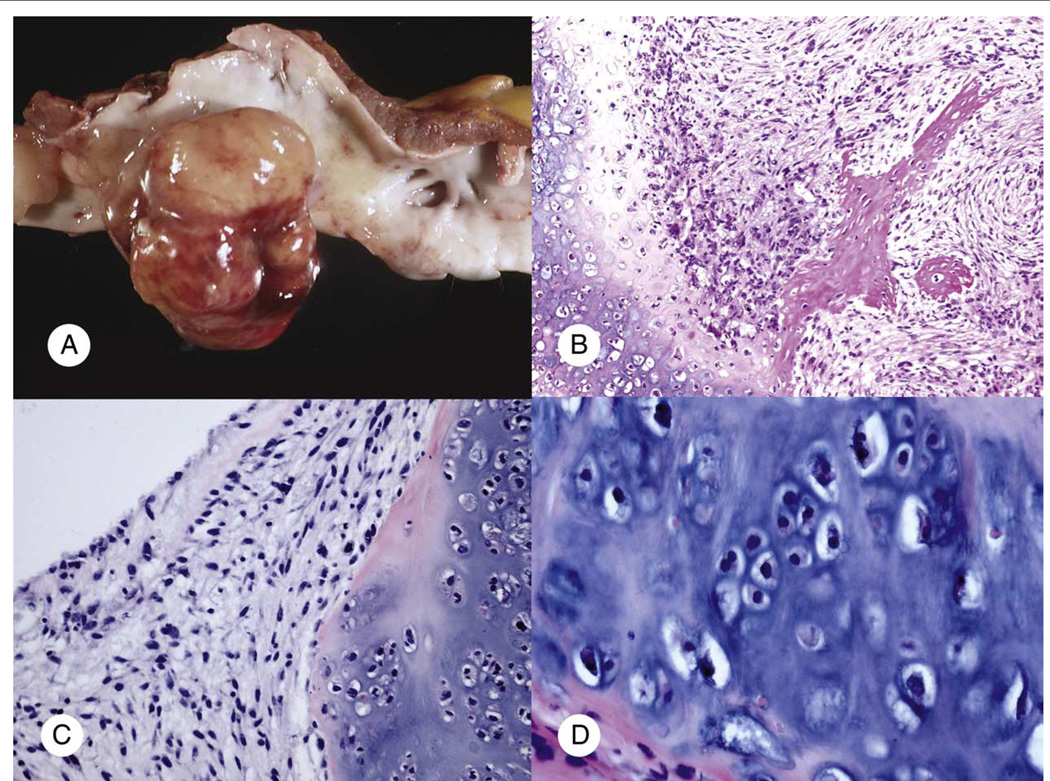
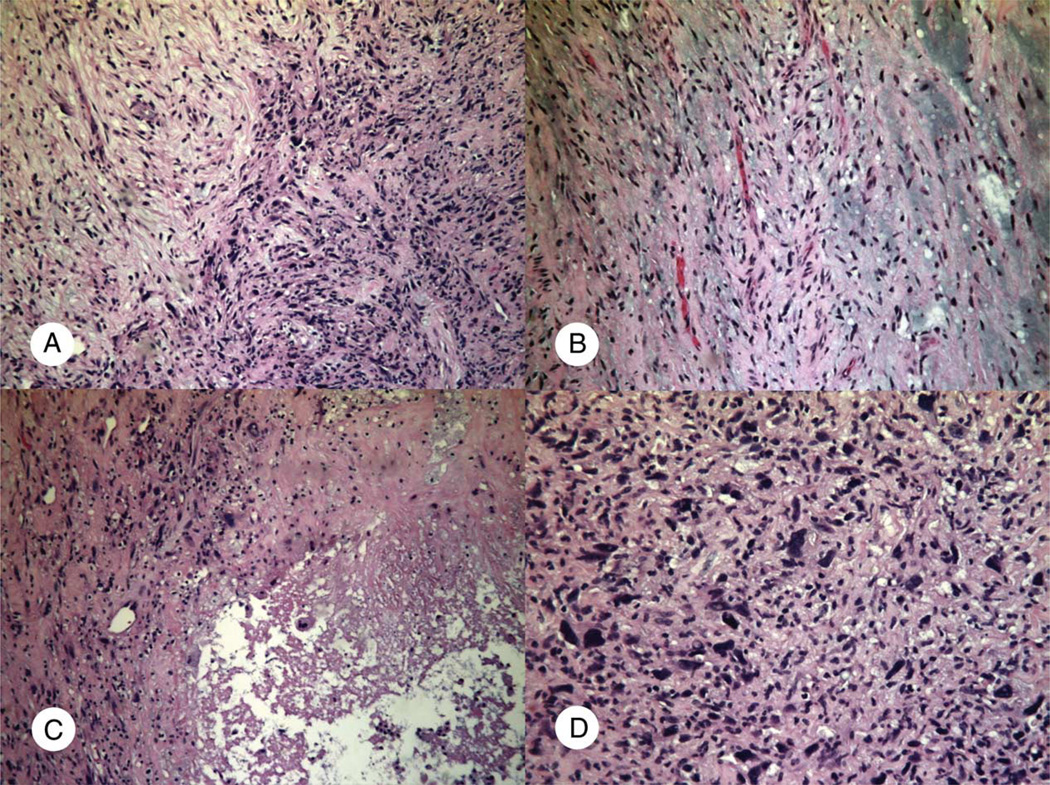
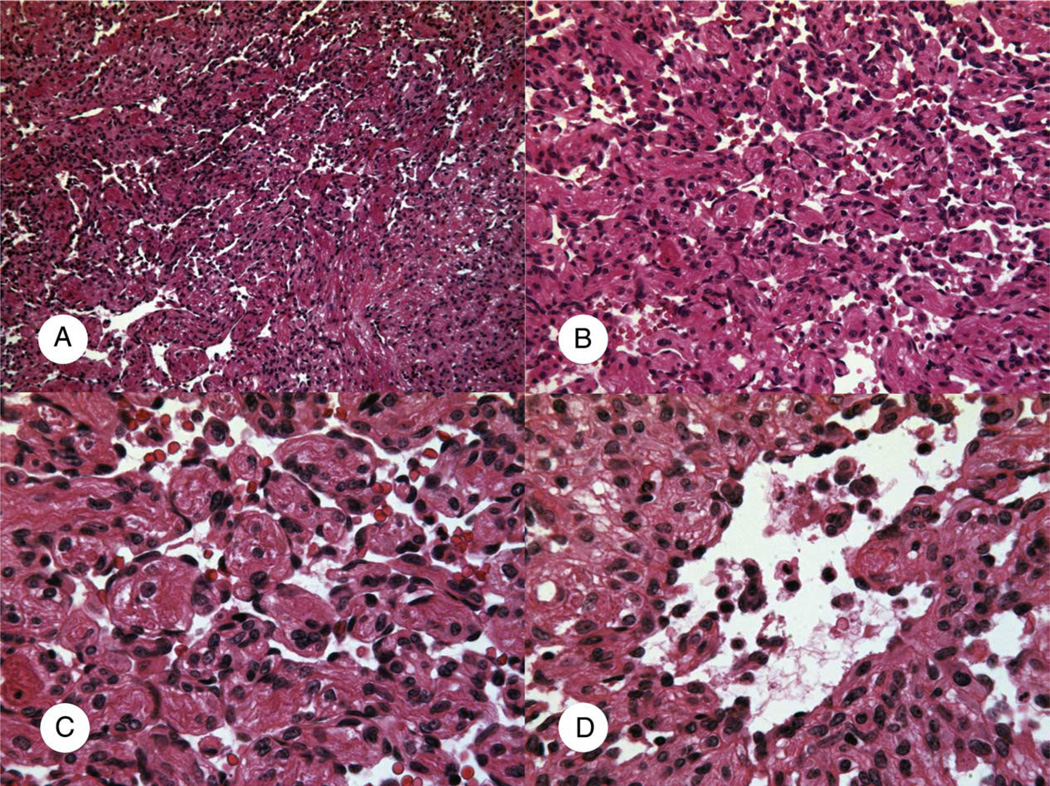
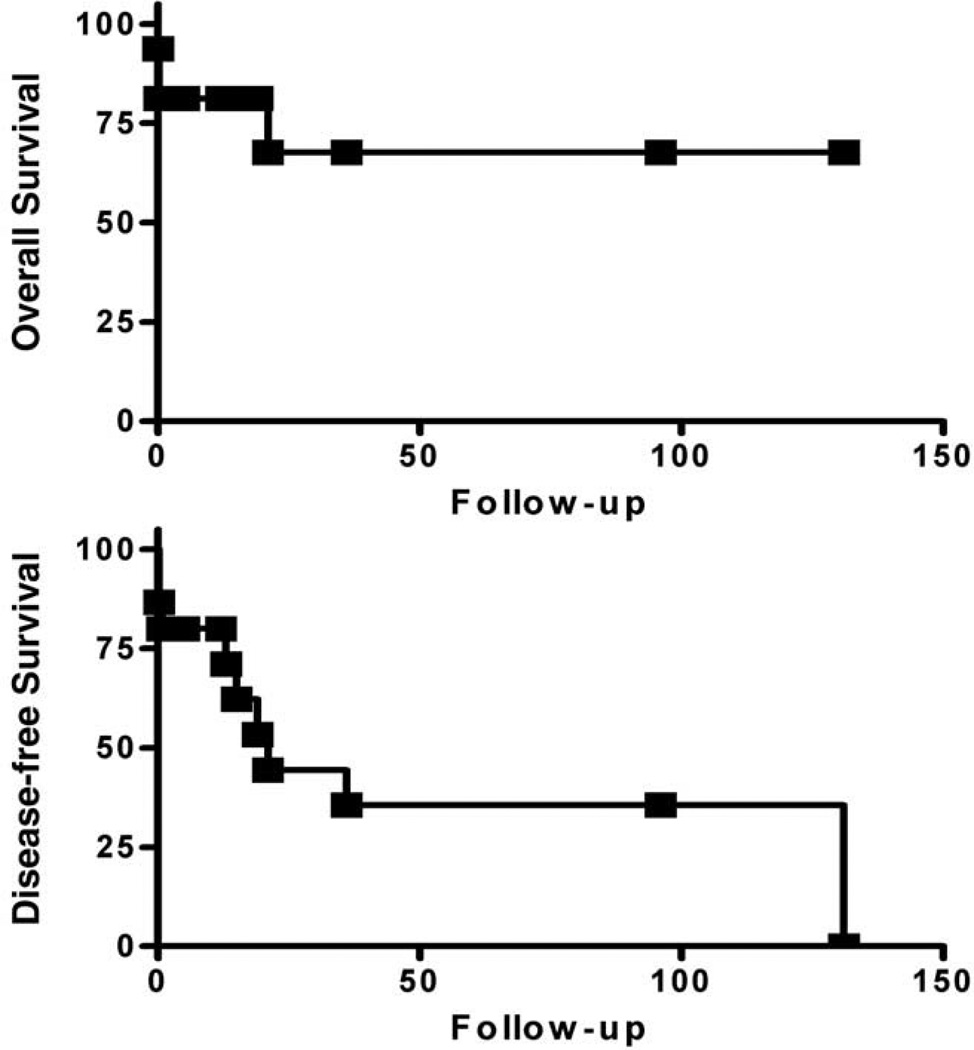
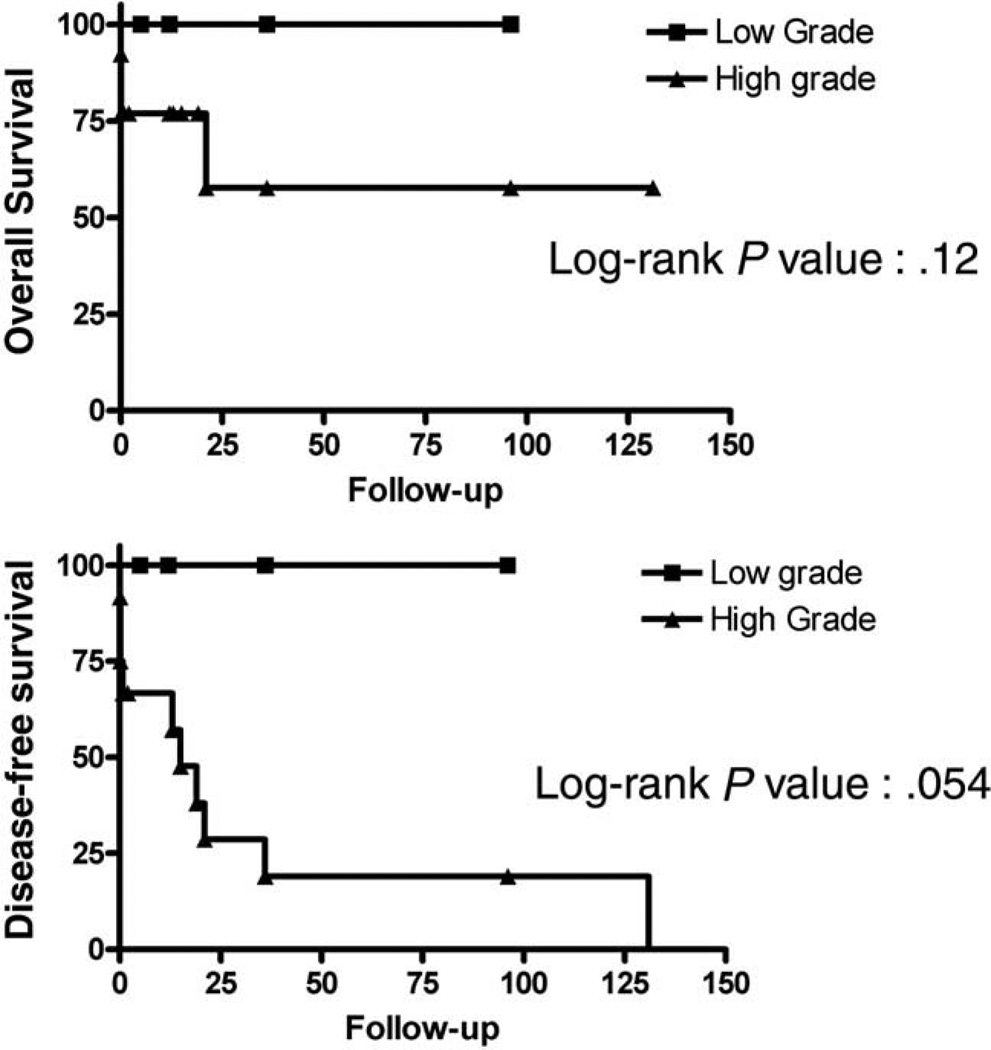
Although cardiac sarcomas are rare in comparison to their soft tissue counterparts, they are the second most common type of primary cardiac neoplasm. Of the few hundred cases reported, most has been based on autopsy series. A series of 27 cardiac sarcomas removed at surgery for curative and diagnostic intent were reviewed for clinicopathologic features with correlation to available postoperative follow-up data in 17 patients. There were 6 angiosarcomas, 6 myxofibrosarcomas, 3 malignant peripheral nerve sheath tumors, 3 leiomyosarcomas, 2 synovial sarcomas, 1 epithelioid hemangioendothelioma, 1 chondrosarcoma, 1 osteosarcoma, and 4 poorly differentiated sarcomas. There was a wide age and size range with slight female predilection. There were 20 cases that arose in the atria/pulmonary vessels, 4 in the ventricles, 1 in mitral valve, and 2 in epi/pericardium. There was a slight left predilection. The histologic grade was low in 4, moderate in 3, and high in 20 cases. Six high-grade and 1 low-grade tumors were also treated with adjuvant chemotherapy and/or radiation. In 17 patients with follow-up data, 6 of 12 patients with high-grade tumor died (4 within 5 days of the initial surgery, 1 in 21 months, and 1 in 131 months), and 1 patient with moderate-grade tumor and all 4 patients with low-grade tumor were alive without evidence of disease at the end of follow-up. Tumor grade appeared to be prognostically important in cardiac sarcoma. Long survival was achieved in patients who survived the initial surgery well.
Figures
References
-
- Mcallister HA, Fenoglio JJ., Jr . Atlas of tumor pathology, 2nd series, fascicle 15. Washington, D.C.: Armed Forces Institute of Pathology, ARP Press; 1978. Tumors of the cardiovascular system; pp. 81–102.
-
- Weiss SW, Goldblum JR. General considerations. In: Weiss SW, Goldblum JR, editors. Soft tissue tumors. 4th ed. St. Louis: C.V. Mosby Co; 2001. pp. 1–18.
-
- Burke AP, Cowan D, Virmani R. Primary sarcomas of the heart. Cancer. 1992;69:387–395. - PubMed
-
- Hausheer FH, Josephson RA, Grochow LB, Weissman D, Brinker JA, Weisman HF. Intracardiac sarcoma diagnosed by left ventricular endomyocardial biopsy. Chest. 1987;92:177–179. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
