

The relative abuse liability of oral oxycodone, hydrocodone and hydromorphone assessed in prescription opioid abusers
- PMID: 18606504
- PMCID: PMC2668197
- DOI: 10.1016/j.drugalcdep.2008.05.007
The relative abuse liability of oral oxycodone, hydrocodone and hydromorphone assessed in prescription opioid abusers
Abstract
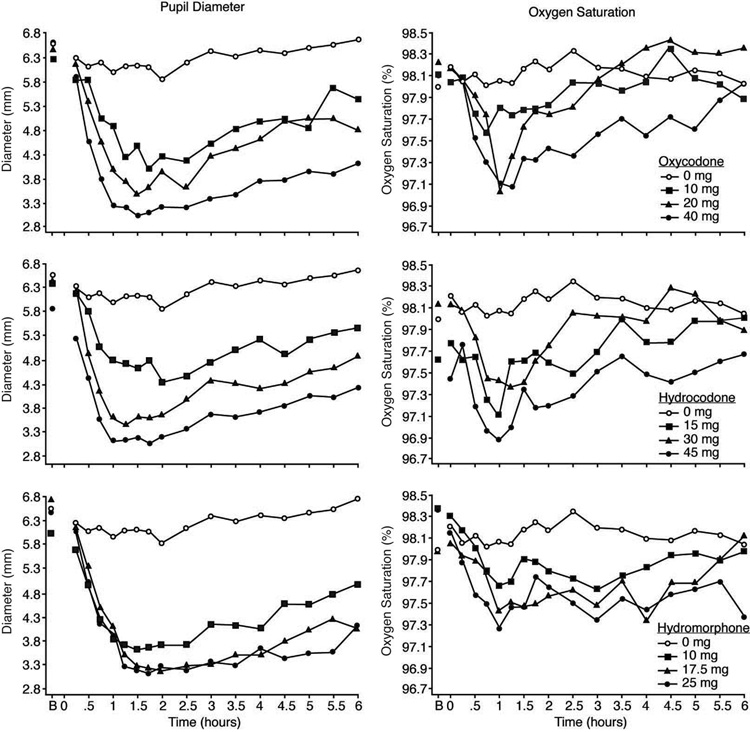
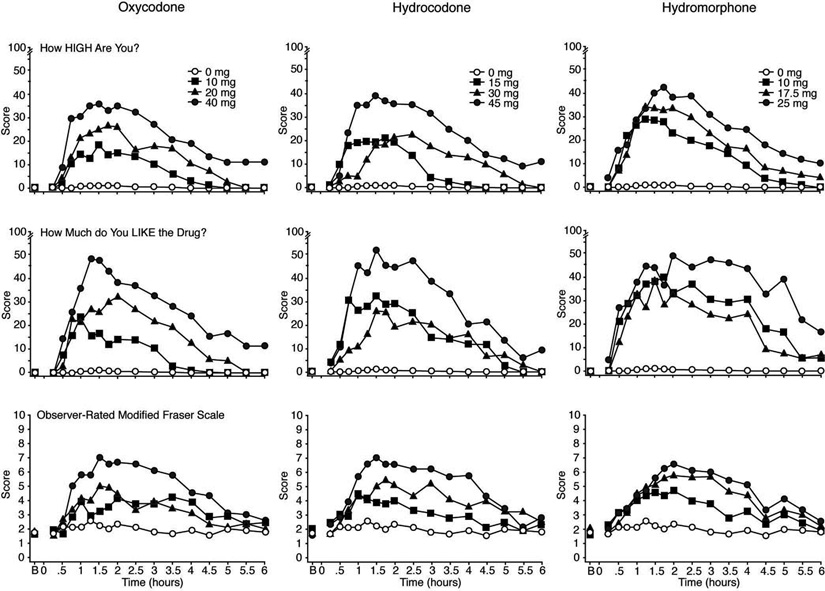
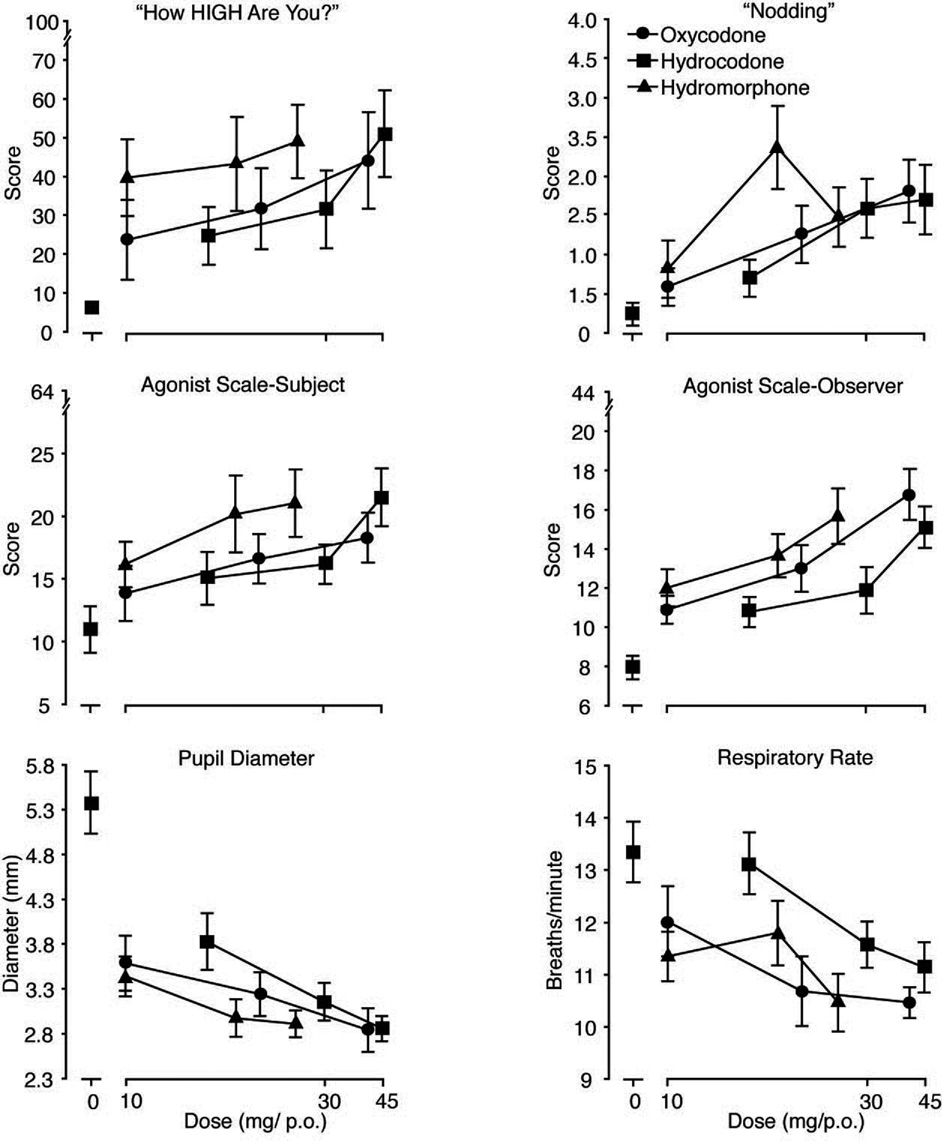
Abuse of prescription opioids has risen precipitously in the United States. Few controlled comparisons of the abuse liability of the most commonly abused opioids have been conducted. This outpatient study employed a double-blind, randomized, within-subject, placebo-controlled design to examine the relative abuse potential and potency of oral oxycodone (10, 20 and 40 mg), hydrocodone (15, 30 and 45 mg), hydromorphone (10, 17.5 and 25mg) and placebo. Healthy adult volunteers (n=9) with sporadic prescription opioid abuse participated in 11 experimental sessions (6.5h in duration) conducted in a hospital setting. All three opioids produced a typical mu opioid agonist profile of subjective (increased ratings of liking, good effects, high and opiate symptoms), observer-rated, and physiological effects (miosis, modest respiratory depression, exophoria and decrements in visual threshold discrimination) that were generally dose-related. Valid relative potency assays revealed that oxycodone was roughly equipotent to or slightly more potent than hydrocodone. Hydromorphone was only modestly more potent (less than two-fold) than either hydrocodone or oxycodone, which is inconsistent with prior estimates arising from analgesic studies. These data suggest that the abuse liability profile and relative potency of these three commonly used opioids do not differ substantially from one another and suggest that analgesic potencies may not accurately reflect relative differences in abuse liability of prescription opioids.
Figures
References
-
- Abreu ME, Bigelow GE, Fleisher L, Walsh SL. Effect of intravenous injection speed on responses to cocaine and hydromorphone in humans. Psychopharmacol. 2001;154:76–84. - PubMed
-
- American Pain Society. Principles of Analgesic Use in the Treatment of Acute Pain and Cancer Pain. Fourth Edition. Glenview, IL: American Pain Society; 1999.
-
- Angst MS, Drover DR, Lotsch J, Ramaswamy B, Naidu S, Wada R, Stanski DR. Pharmacodynamics of orally administered sustained-release hydromorphone in humans. Anesthesiology. 2001;94:63–73. - PubMed
-
- Beaver WT, Wallenstein SL, Rogers A, Houde RW. Analgesic studies of codeine and oxycodone in patients with cancer; II: Comparisons of intramuscular oxycodone with intramuscular morphine and codeine. J Pharmacol Exp Ther. 1978;207:101–108. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
