

Marked regional left ventricular heterogeneity in hypertensive left ventricular hypertrophy patients: a losartan intervention for endpoint reduction in hypertension (LIFE) cardiovascular magnetic resonance and echocardiographic substudy
- PMID: 18606908
- PMCID: PMC2693884
- DOI: 10.1161/HYPERTENSIONAHA.108.109819
Marked regional left ventricular heterogeneity in hypertensive left ventricular hypertrophy patients: a losartan intervention for endpoint reduction in hypertension (LIFE) cardiovascular magnetic resonance and echocardiographic substudy
Abstract
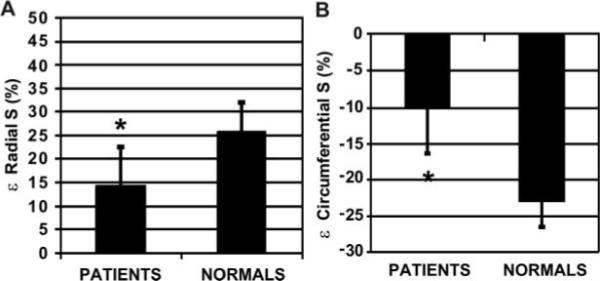
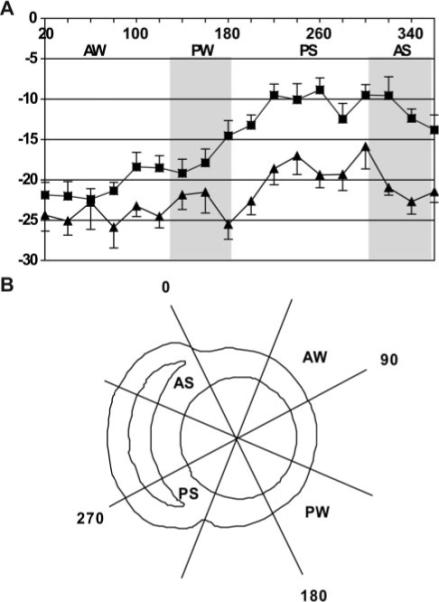
Concentric hypertensive left ventricular (LV) hypertrophy is presumed to be a symmetrical process. Using MRI-derived intramyocardial strain, we sought to determine whether segmental deformation was also symmetrical, as suggested by echocardiography. High echocardiographic LV relative wall thickness in hypertensive LV hypertrophy allows preserved endocardial excursion despite depressed LV midwall shortening (MWS). Depressed MWS is an adverse prognostic indicator, but whether this is related to global or regional myocardial depression is unknown. We prospectively compared MWS derived from linear echocardiographic dimensions with MR strain(in) in septal and posterior locations in 27 subjects with ECG LV hypertrophy in the Losartan Intervention for Endpoint Reduction in Hypertension Study. Although MRI-derived mass was higher in patients than in normal control subjects (124.0+/-38.6 versus 60.5+/-13.2g/m(2); P<0.001), fractional shortening (30+/-5% versus 33+/-3%) and end-systolic stress (175+/-22 versus 146+/-28 g/cm(2)) did not differ between groups. However, mean MR(in) was decreased in patients versus normal control subjects (13.9+/-6.8% versus 22.4+/-3.5%), as was echo MWS (13.4+/-2.8% versus 18.2+/-1.4%; both P<0.001). For patients versus normal control subjects, posterior wall(in) was not different (17.8+/-7.1% versus 21.6+/-4.0%), whereas septal(in) was markedly depressed (10.1+/-6.6% versus 23.2+/-3.4%; P<0.001). Although global MWS by echocardiography or MRI is depressed in hypertensive LV hypertrophy, MRI tissue tagging demonstrates substantial regional intramyocardial strain(in) heterogeneity, with most severely depressed strain patterns in the septum. Although posterior wall 2D principal strain was inversely related to radius of curvature, septal strain was not, suggesting that factors other than afterload are responsible for pronounced myocardial strain heterogeneity in concentric hypertrophy.
Figures
References
-
- Koren MJ, Devereux RB, Casale PN, Savage DD, Laragh JH. Relation of left ventricular mass and geometry to morbidity and mortality in uncomplicated essential hypertension. Ann Int Med. 1991;114:345–352. - PubMed
-
- de Simone G, Devereux RB, Koren MJ, Mensah GA, Casale PN, Laragh JH. Midwall left ventricular mechanics. An independent predictor of cardiovascular risk in arterial hypertension. Circulation. 1996;93:259–265. - PubMed
-
- Levy D, Garrison RJ, Savage DD, Kannel WB, Castelli WP. Prognostic implications of echocardiographically determined left ventricular mass in the Framingham Heart Study. N Engl J Med. 1990;322:1561–1566. - PubMed
-
- Aurigemma GP, Silver KH, Priest MA, Gaasch WH. Geometric changes allow normal ejection fraction despite depressed myocardial shortening in left ventricular hypertrophy. J Am Coll Cardiol. 1995;26:195–202. - PubMed
-
- de Simone G, Devereux RB, Roman MJ, Ganau A, Saba PS, Alderman MH, Laragh JH. Assessment of left ventricular function by the midwall fractional shortening/end-systolic stress relation in human hypertension. J Am Coll Cardiol. 1994;23:1444–1451. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
