

A panel of kallikrein markers can reduce unnecessary biopsy for prostate cancer: data from the European Randomized Study of Prostate Cancer Screening in Göteborg, Sweden
- PMID: 18611265
- PMCID: PMC2474851
- DOI: 10.1186/1741-7015-6-19
A panel of kallikrein markers can reduce unnecessary biopsy for prostate cancer: data from the European Randomized Study of Prostate Cancer Screening in Göteborg, Sweden
Abstract
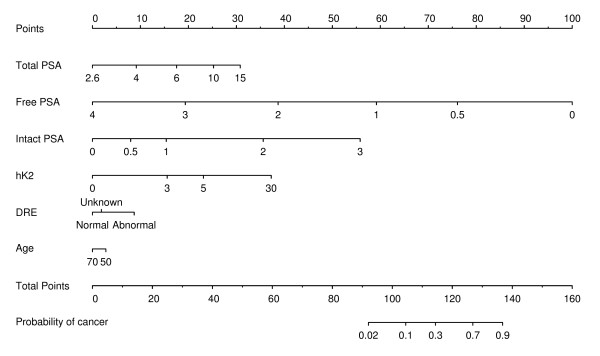
Background: Prostate-specific antigen (PSA) is widely used to detect prostate cancer. The low positive predictive value of elevated PSA results in large numbers of unnecessary prostate biopsies. We set out to determine whether a multivariable model including four kallikrein forms (total, free, and intact PSA, and human kallikrein 2 (hK2)) could predict prostate biopsy outcome in previously unscreened men with elevated total PSA.
Methods: The study cohort comprised 740 men in Göteborg, Sweden, undergoing biopsy during the first round of the European Randomized study of Screening for Prostate Cancer. We calculated the area-under-the-curve (AUC) for predicting prostate cancer at biopsy. AUCs for a model including age and PSA (the 'laboratory' model) and age, PSA and digital rectal exam (the 'clinical' model) were compared with those for models that also included additional kallikreins.
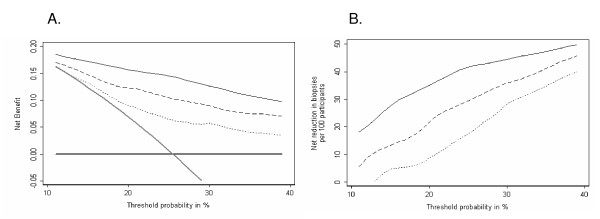
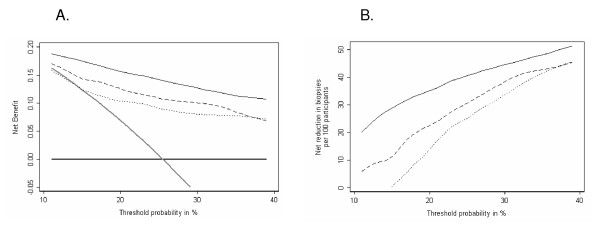
Results: Addition of free and intact PSA and hK2 improved AUC from 0.68 to 0.83 and from 0.72 to 0.84, for the laboratory and clinical models respectively. Using a 20% risk of prostate cancer as the threshold for biopsy would have reduced the number of biopsies by 424 (57%) and missed only 31 out of 152 low-grade and 3 out of 40 high-grade cancers.
Conclusion: Multiple kallikrein forms measured in blood can predict the result of biopsy in previously unscreened men with elevated PSA. A multivariable model can determine which men should be advised to undergo biopsy and which might be advised to continue screening, but defer biopsy until there was stronger evidence of malignancy.
Figures
References
-
- Fadare O, Wang S, Mariappan MR. Practice patterns of clinicians following isolated diagnoses of atypical small acinar proliferation on prostate biopsy specimens. Arch Pathol Lab Med. 2004;128:557–560. - PubMed
-
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Smigal C, Thun MJ. Cancer statistics, 2006. CA Cancer J Clin. 2006;56:106–130. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
